Non-Surgical Repair of Patellar Tendonitis with Autologous Platelet Concentrate Using Ultrasound Guidance: Two Case Reports
Beacon Orthopedic & Sports Medicine, Cincinnati, OH
Case 1 – 26 y/o Male with Chronic Left Patellar Tendonitis Clinical History: A 26 year old professional male basketball player presented with a 4 year history of chronic left patellar tendonitis initially diagnosed by MRI while he was playing in college. This was treated with various non-steroidal anti-inflammatory medications, physical therapy, tendon strapping, iontophoresis, and relative rest. The patient gained no significant relief from these treatments. Physical Examination: Physical examination revealed full range of motion of the knee with excellent flexibility of the quadriceps and hamstrings. No effusion was noted. The cruciate and collateral ligaments were intact; no joint line tenderness was noted. The patellar tendon revealed point tenderness at the inferior pole of the patella. Pain was reproduced with resisted extension of the knee at 90 degrees flexion as well as with one-legged hops. X-rays- 3 views including standing AP, lateral, and merchants revealed no acute abnormality. Diagnostic MSK ultrasound was performed using the 12MgHz probe and revealed significant thickening of the tendon proximally and an area of anechogenicity consistent with mucoid degeneration (Fig.1-A). The opposite patellar tendon appeared normal (Fig.1-B). Description of Procedure:
• Left Knee sterilely prepped and draped • 3cc of Platelet Rich Plasma (PRP) was prepared from 20cc of whole blood (SmartPReP
System, Harvest Technologies Corp., Plymouth, MA).
• 4cc 2% xylocaine with 1:100,000 dilution of epinephrine was injected into the tendon to
fenestrate the area of chronic tendonosis and to help activate the platelets.
• 3cc of PRP was injected into the thickened area of tendonosis • 1cc of Bovine Thrombin with Calcium Chloride (CaCl) was then injected to create a
A second identical procedure was preformed two weeks later. Two weeks after the second injection the tendon was no longer tender to palpation, nor was there pain with resisted extension of the knee. Physical Therapy: Physical therapy was started and consisted of stretching, eccentric strengthening, and cardiovascular conditioning. After four weeks of therapy including a functional return to basketball, the patient was able to play the entire professional season pain free. Patient Follow-Up: Repeat MSK ultrasound was performed 16 weeks after the final injection. The tendon was significantly less thickened and the area of anechogenicity was no longer visible (Fig.2). Case 2 – 20 y/o Female with Patellar Tendonitis
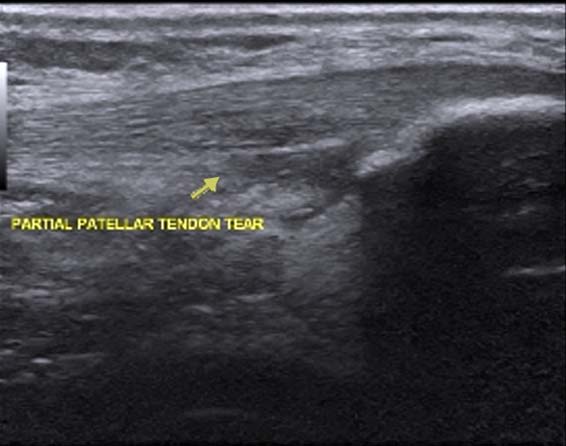
Clinical History: A 20 year old female Division 1 collegiate basketball player presented with a 6 month history of patellar tendonitis diagnosed by point tenderness at the inferior pole of the right patella. This was treated with ice, modalities including iontophoresis, NSAIDS, physical therapy and activity modification. The patient was for the most part able to play through the pain. Six months after being diagnosed with patellar tendonitis, the patient sustained a valgus blow to the knee in the flexed position and was found by MRI to have an acute, partial tear of the patellar tendon superimposed on chronic tendonosis (Fig.3). Physical Examination: Physical examination revealed full range of motion of the knee with fair flexibility of hamstrings and quadriceps with no atrophy noted. The patient was point tender at the inferior pole of the patellar with pain present upon resisted extension of knee. The remainder of the knee exam was WNL. Diagnostic MSK ultrasound revealed thickening of the tendon proximally beginning at the inferior pole the patella and an area of anechogenicity corresponding to area of high signal intensity on MRI scan (Fig.4). Description of Procedure:
• Right Knee sterilely prepped and draped • 3cc of Platelet Rich Plasma (PRP) was prepared from 20cc of whole blood (SmartPReP
System, Harvest Technologies Corp., Plymouth, MA).
• 4cc 2% xylocaine with 1:100,000 dilution of epinephrine was injected into the tendon to
fenestrate the area of chronic tendonosis and to activate the platelets.
• 3cc of PRP was injected into the thickened area of tendonosis and the area of acute
• 1cc of Bovine Thrombin with CaCl was then injected to create a lasting platelet plug
The identical procedure was repeated in 3 weeks. The 4ccs of PRP were this time injected into the area of chronic tendonosis and thrombin was not used as the area of partial tearing had shown significant healing. Patient Follow-Up Three weeks after the second injection, the tendon was no longer tender to palpation, nor was there pain with resisted extension of the knee. Physical therapy was started and consisted of stretching, eccentric strengthening, and cardiovascular conditioning. After three weeks of therapy including a functional return to basketball, the patient was able to return to basketball with no anterior knee pain or limitations. Twelve weeks after the second PRP injection, repeat MSK ultrasound was performed and the area of partial tendon appeared to be healed. The chronic area of tendonosis appeared less thickened and normal tendon striations were noted (Fig.5). Discussion: Chronic patellar tendonitis is a very difficult condition to treat. The patellar tendon is a weight bearing tendon and therefore corticosteroid injections are contraindicated and surgery is often unsuccessful. The most common presenting symptom is pain with jumping activities and therefore is most common in athletes who are involved in basketball and volleyball. Relative rest, ice, NSAIDS, iontophoresis, and other physical therapy modalities offer little relief. PRP with ultrasound guided needle placement to allow precise placement of the tissue graft offers a very simple and safe treatment modality that not only alleviates the pain, but replaces the mucoid degeneration within the tendon with healthy tendon as illustrated above thereby allowing the athlete a safe and pain free return to sports.
Merkblatt zum Kopflausbefall in Gemeinschaftseinrichtungen in der Gemeinschaftseinrichtung, die Ihr Kind besucht, sind Kopfläuse aufgetreten. Vielleicht ist Ihr Kind sogar selbst betroffen. Kopflausbefall ist lästig und unangenehm. Bei engem Kontakt ist die Gefahr einer Weiterverbreitung durch das Überwandern der Läuse von Kopf zu Kopf bzw. gelegentlich über die Kleidung sehr groß. Um die

 Non-Surgical Repair of Patellar Tendonitis with Autologous Platelet
Non-Surgical Repair of Patellar Tendonitis with Autologous Platelet 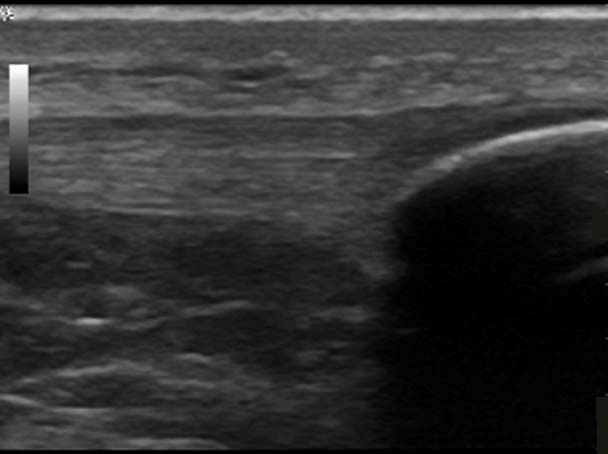 Description of Procedure:
Description of Procedure: 
 Case 2 – 20 y/o Female with Patellar Tendonitis
Case 2 – 20 y/o Female with Patellar Tendonitis 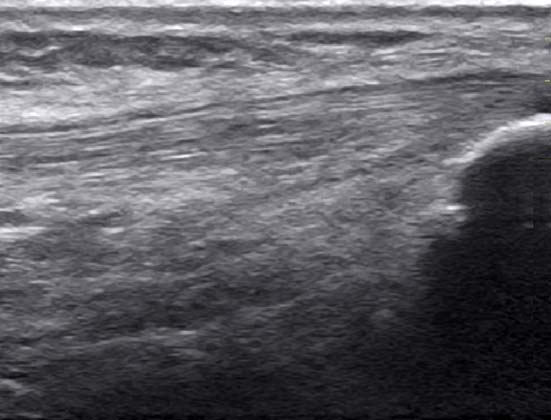 The identical procedure was repeated in 3 weeks. The 4ccs of PRP were this time injected into
The identical procedure was repeated in 3 weeks. The 4ccs of PRP were this time injected into