FERTILITY AND STERILITY VOL. 77, NO. 1, JANUARY 2002Copyright 2002 American Society for Reproductive MedicinePublished by Elsevier Science Inc. Printed on acid-free paper in U.S.A. A nomogram to predict the probability of live birth after clomiphene citrate induction of ovulation in normogonadotropic oligoamenorrheic infertility Babak Imani, M.D.,a Marinus J. C. Eijkemans, M.Sc.,b Egbert R. te Velde, M.D., Ph.D.,cJ. Dik F. Habbema, M.D., Ph.D.,b and Bart C. J. M. Fauser, M.D., Ph.D.a
Division of Reproductive Medicine, Department of Obstetrics and Gynecology, Erasmus University MedicalCenter of Rotterdam, Rotterdam, The NetherlandsObjective: To establish whether initial screening characteristics of normogonadotropic anovulatory infertile women can aid in predicting live birth after induction of ovulation with clomiphene citrate (CC). Design: Prospective longitudinal single-center study. Setting: Specialist academic fertility unit. Patient(s): Two hundred fifty-nine couples with a history of infertility, oligoamenorrhea, and normal follicle-stimulating hormone (FSH) concentrations who have not been previously treated with any ovulation- Intervention(s): 50, 100, or 150 mg of oral CC per day, for 5 subsequent days per cycle. Main Outcome Measure(s): Conception leading to live birth after CC administration. Result(s): After receiving CC, 98 (38%) women conceived, leading to live birth. The cumulative live birth
rate within 12 months was 42% for the total study population and 56% for the ovulatory women who had
received CC. Factors predicting the chances for live birth included free androgen index (testosterone/sex
hormone– binding globulin ratio), body mass index, cycle history (oligomenorrhea versus amenorrhea), and
Reprint requests: BartC. J. M. Fauser, M.D.,
Conclusion(s): It is possible to predict the individual chances of live birth after CC administration using two
distinct prediction models combined in a nomogram. Applying this nomogram in the clinic may be a step
forward in optimizing the decision-making process in the treatment of normogonadotropic anovulatory
infertility. Alternative first line of treatment options could be considered for some women who have limited
chances for success. (Fertil Steril 2002;77:91–7. 2002 by American Society for Reproductive Medicine.)
University Medical Centerof Rotterdam, Dr. Key Words: Infertility, female, human, follow-up studies, anovulation, polycystic ovary syndrome, predic-
tion, induction of ovulation, clomiphene citrate
GD Rotterdam, TheNetherlands (FAX: 31-10-436-7306; E-mail:
approximately 50% will conceive within six
cause of female infertility. In most women,
normal serum follicle-stimulating hormone
(FSH) concentrations are found. Since its in-
induction of ovulation has been the subject of
troduction (1), clomiphene citrate (CC) has
been used worldwide as the first-choice medi-
several investigations, all of which focused on
Health, Erasmus UniversityMedical Center of
cation in the treatment of anovulatory infertil-
the entire group of anovulatory patients who
ity. Since the early 1970s, CC treatment has
start with CC therapy (5–11). These investiga-
been restricted to normogonadotropic oligoam-
tors have failed to identify predictors of CC
and Gynecology, UniversityHospital of Utrecht,
enorrheic infertility (WHO group 2) (2). A
treatment outcome. In contrast, our group fo-
significant proportion of these women, how-
cused on prediction of ovulation and concep-
ever, remain anovulatory after receiving CC
tion separately (3, 4). This approach in life-
0015-0282/02/$22.00PII S0015-0282(01)02929-6
medication. Of 75% ovulatory CC patients,
table analysis for prediction of pregnancy
chances seems mandatory for the following statistical rea-
enorrhea (bleeding interval Ͼ 6 months), [2] serum FSH
sons. Discontinuation of CC therapy due to persistent anovu-
levels within normal limits (1–10 IU/L) (2, 13), [3] normal
lation is clearly an informative selective drop-out, because
serum prolactin and thyroid-stimulating hormone levels, [4]
chances for CC treatment outcome are different for this
spontaneous menses or positive bleeding response to proges-
group when compared with women who continue CC ther-
togen withdrawal, [5] BMI (weight divided by the square of
apy. Therefore, inclusion of both CC responders and CC
the patient’s height) Ͼ18 kg/m2, [6] age between 19 and 40
nonresponders in a life-table analysis for prediction of con-
years, [7] no previous use of ovulation-induction agents, [8]
a total motile sperm count (TMC ϭ ejaculate volume [mil-
We developed two distinct prediction models applying
liliters] ϫ sperm concentration [106/mL] ϫ percentage of
multivariate analyses (3, 4). The first model predicts ovarian
progressive motile sperm) of the partner above 1 million, [9]
response after CC in the entire group of anovulatory patients
negative history of any tubal pathology, and, finally, [10] no
on the basis of initial screening characteristics, such as free
indication for intrauterine insemination. Institutional review
androgen index (testosterone/sex hormone– binding globulin
board approval was obtained from the human subjects com-
ratio), body mass index (BMI), cycle history (oligomenor-
mittee of the Erasmus University Medical Center of Rotter-
rhea versus amenorrhea), and mean ovarian volume (3, 12).
dam and informed consent was obtained from all study
The second model predicts the chances of conception exclu-
sively among those women who have reached ovulatory
The standardized initial clinical, sonographic, and endo-
cycles after CC administration, and includes the woman’s
crine screening took place prior to the initiation of CC
age and cycle history (4). Although scientifically sound, this
ovulation induction, as had been described previously
approach seems difficult to apply in the daily clinical prac-
(3, 4, 12). The clinical screening included the patient’s age,
tice. Moreover, the question remains unanswered whether
type of infertility, cycle history, BMI, waist-to-hip ratio
the chances of having a live birth after CC administration can
(WHR), and previous medication and/or surgery. Transvag-
be predicted prior to the initiation of medication. By com-
inal sonography included assessment of the ovarian stroma
bining both prediction models, a nomogram may be devel-
echogenicity (arbitrarily classified from 1 to 3 per ovary),
oped that predicts the chances of a given anovulatory patient
ovarian volume (in milliliters), and total number of follicles
to conceive and obtain a live birth after the CC protocol.
(both ovaries), as has been described previously (14, 15).
Anovulatory patients present with a wide range of
The sonographic monitoring was performed by a single
chances to conceive after CC administration. This may be
observer (B.I.). Endocrine screening included serum assays
due to differences in the underlying ovarian abnormalities,
to determine the levels of FSH, luteinizing hormone (LH),
the patient’s age, the body weight, and the individual differ-
estradiol, androstenedione (AD), testosterone (T), sex hor-
ences in the anti-estrogenic effects of CC on cervical mucus
mone– binding globulin (SHBG), fasting insulin and glu-
or endometrium. Applying a nomogram in the clinic may
cose, free and total insulin-like growth factor-I (IGF-I),
render the ovulation-induction protocols more patient-
inhibin B, and leptin concentrations, as has been described
tailored and more cost-effective. Patients with a poor pre-
previously (12). Hormone assays used and the intra-assay
dicted chance to conceive could be advised to refrain from
and interassay coefficients of variation valid for this study
CC therapy and start with an alternative first-line treatment
have all been described previously (3, 4, 12).
modality such as weight reduction, insulin-sensitizing
The treatment protocol and the assessment of ovarian
agents, or exogenous gonadotropins. Particularly in women
response and conception after CC administration have also
of advanced age, precious time lost in ascertaining that CC
been described previously (3, 4). In brief, the women re-
treatment is ineffective could be used for a more effective
ceived initial CC doses of 50 mg/day starting on cycle day 3
approach as the first-line therapy. We now report the con-
after a spontaneous or progestogen-induced withdrawal
struction of a nomogram to identify the characteristics found
bleeding. In cases of absent ovarian response, the dosage
upon initial screening in a large cohort of normogonado-
was increased to 100 and 150 mg/day in subsequent cycles.
tropic anovulatory infertile women that predicted the indi-
Ovulation after CC medication was assessed by sonographic
vidual chance of pregnancy leading to live birth after CC
monitoring of follicle growth and the finding of midluteal
progesterone levels Ͼ25 nmol/L. Conception was defined asa positive urinary pregnancy test (clearview, hCG II,
Unipath Ltd, Bedford, UK) more than 3 days after theexpected menses. Live birth was defined as delivery of a
Patients and Study Protocol
baby. Information regarding deliveries and the health con-
Between February 1993 and May 1999, 259 women at-
dition of the babies born was collected using the hospital
tending our infertility unit were included in the present study
records. In cases of home delivery, we collected the infor-
using the following inclusion criteria: [1] oligomenorrhea
mation directly from the patient and her general practitioner
(bleeding intervals between 35 days and 6 months) or am-
Imani et al. Data Analysis
The statistical analysis of conception leading to live birth
Eighty-three patients (32%) presented with ovulatory cycles
in anovulatory patients after a CC protocol should take into
account the following two steps: ovulatory response to CC
A total of 111 (43%) women conceived after CC treat-
and conception in case of ovulation. Patients remaining
ment and 11 (10% of conceptions) miscarried. There was
anovulatory after CC are considered to have no chance to
one case of ectopic pregnancy and one case of intrauterine
conceive with this therapy. Therefore, the cumulative rate of
death. A total of 98 (38%) patients had a live birth. Sixty-
conception leading to live birth was calculated by multiply-
seven patients delivered at the hospital and could leave the
ing the chance of achieving ovulation after CC, with the
unit within 24 hours. Nineteen patients were hospitalized for
estimated Kaplan-Meier (16) cumulative probabilities for
prenatal and postnatal care. Four pregnant women required
conception in the group of ovulatory women after the CC
antihypertensive medication. There were no maternal or fetal
deaths. In 15 women an instrumental delivery was per-
We constructed a prediction model of the probability of
formed, and in 13 patients a caesarean section was per-
conception resulting in live birth within 6 months after
formed. At birth, the mean Ϯ SD gestational age was 39.3 Ϯ
initiation of CC ovulation induction by combining the pre-
2.8 weeks, and the mean weight of the babies was 3142 Ϯ
viously published prediction model for the chance of clomi-
590 grams. There were no postpartum deaths in the first year
phene-resistant anovulation (3) with a prediction model for
after the delivery, and no congenital abnormalities were
the probability of conception leading to live birth in ovula-
tory patients after CC administration. The current study
The odds ratios of screening characteristics separately for
differs from the previously published model for predicting
ovulation in the entire population and in women who had
chances for conception (4) with respect to the starting point
live births among the ovulatory CC women are presented in
of follow-up (initiation of CC therapy versus first ovulation
Table 1. Screening characteristics were included on the basis
after CC). To implement these findings in clinical practice,
of statistical significance in previous multivariate analysis
we included months rather than ovulatory cycles and live
predicting ovulation (FAI, BMI, cycle history, ovarian vol-
birth instead of ongoing pregnancy in the current analysis. A
ume, leptin), predicting pregnancy in ovulatory patients (age,
nomogram was constructed by combining the model to pre-
cycle history), and biological relevance for ovarian dysfunc-
dict ovulation in the entire group of women with the model
tion (LH, hyperandrogenemia, insulin, insulin/glucose ratio,
predicting live birth in ovulatory CC patients.
inhibin B, free IGF-I) or pregnancy prediction (infertility
To determine the goodness-of-fit of the combined predic-
history, bleeding interval in case of oligomenorrhea, total
tion model, patients were divided into five equal groups
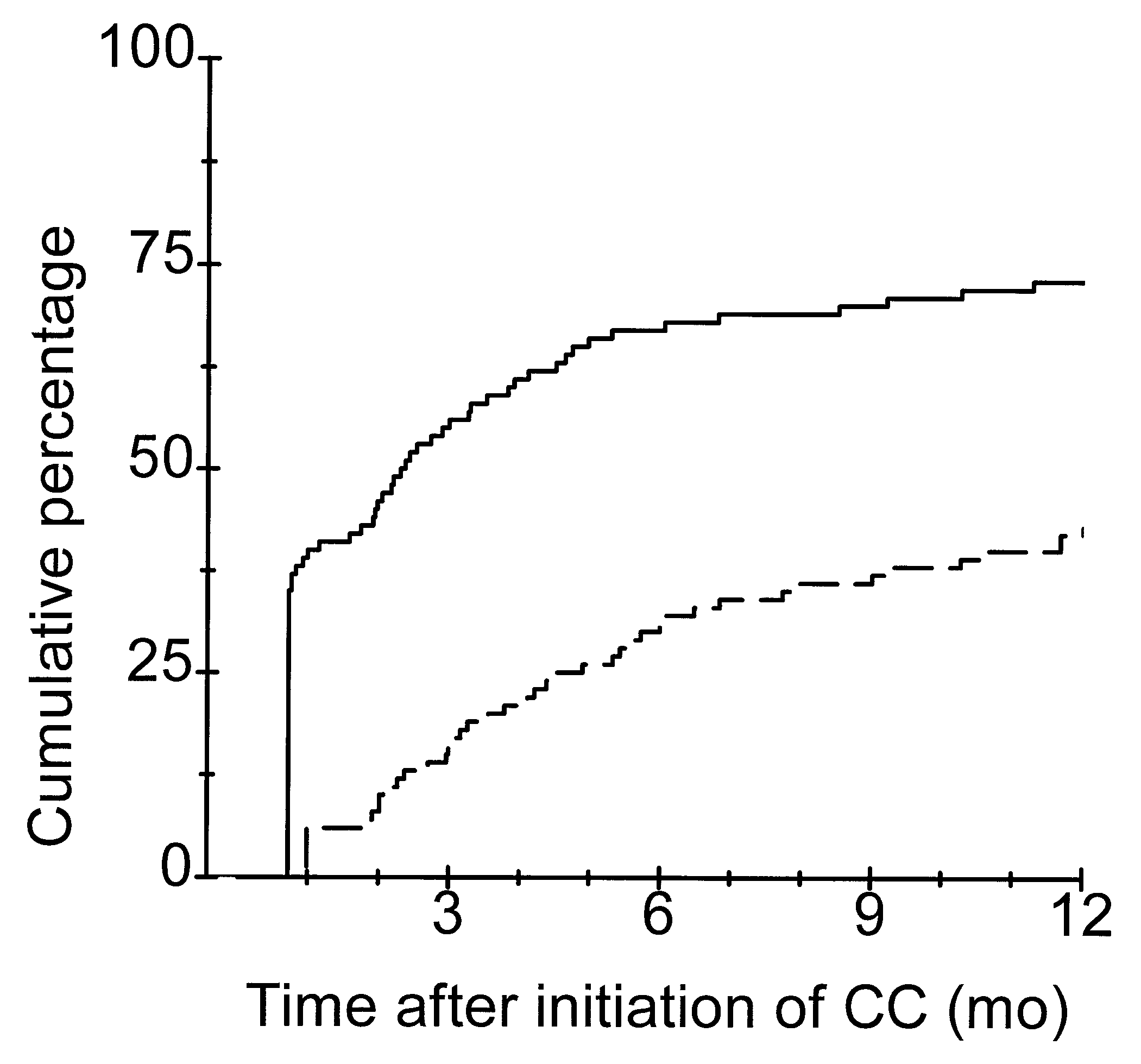
motile sperm count). The cumulative rates of first ovulation
according to quintiles of the predicted probability of concep-
and first conception ending in live birth are depicted in
tion leading to live birth. Using a chi-square test, the mean
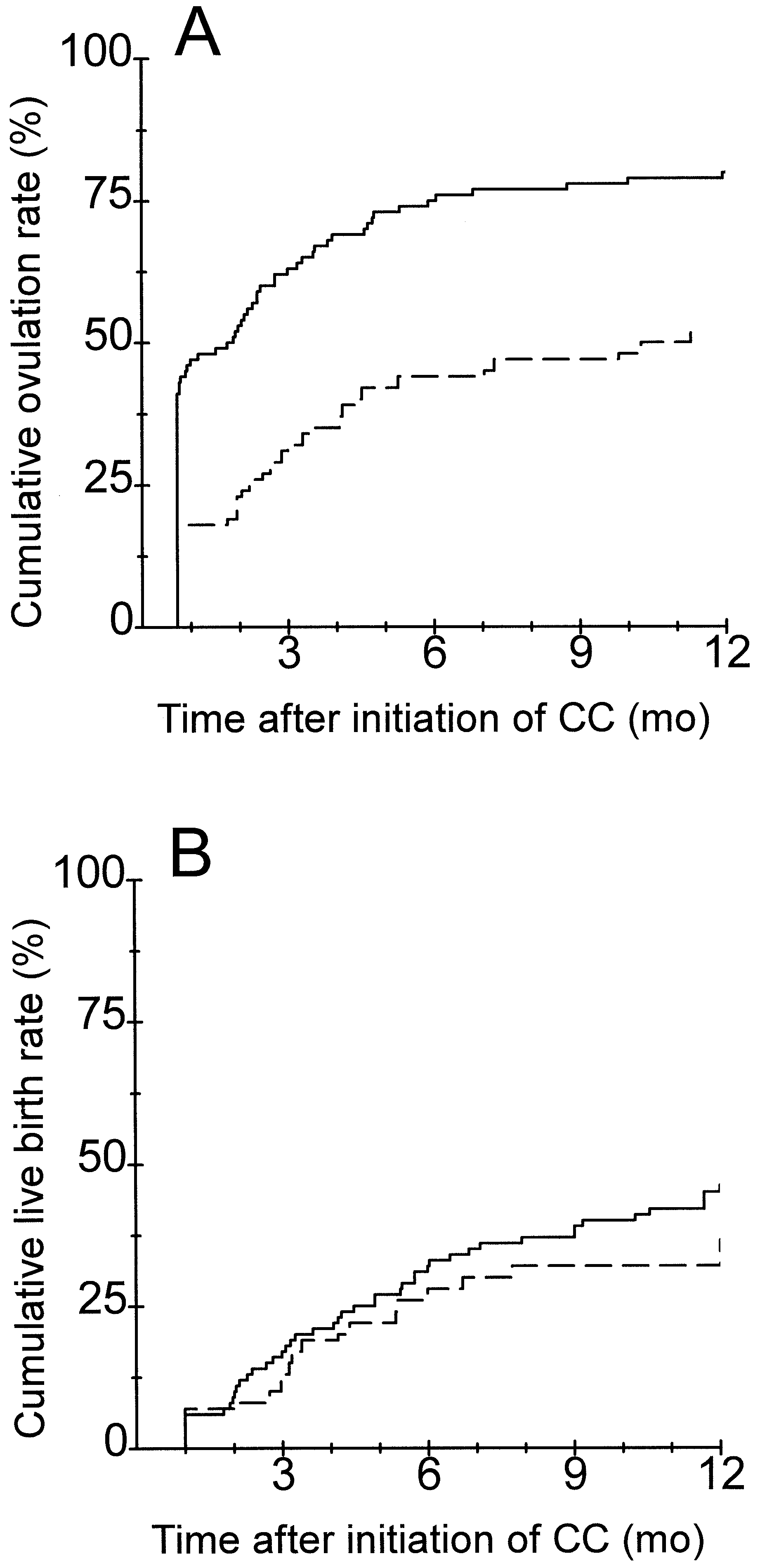
Figure 1. The impact of cycle history on cumulative ovula-
predicted probability within each group was compared with
tion and live birth rates after CC treatment is depicted in
the observed probability, calculated by the Kaplan-Meier
method described in the previous paragraph. Data were
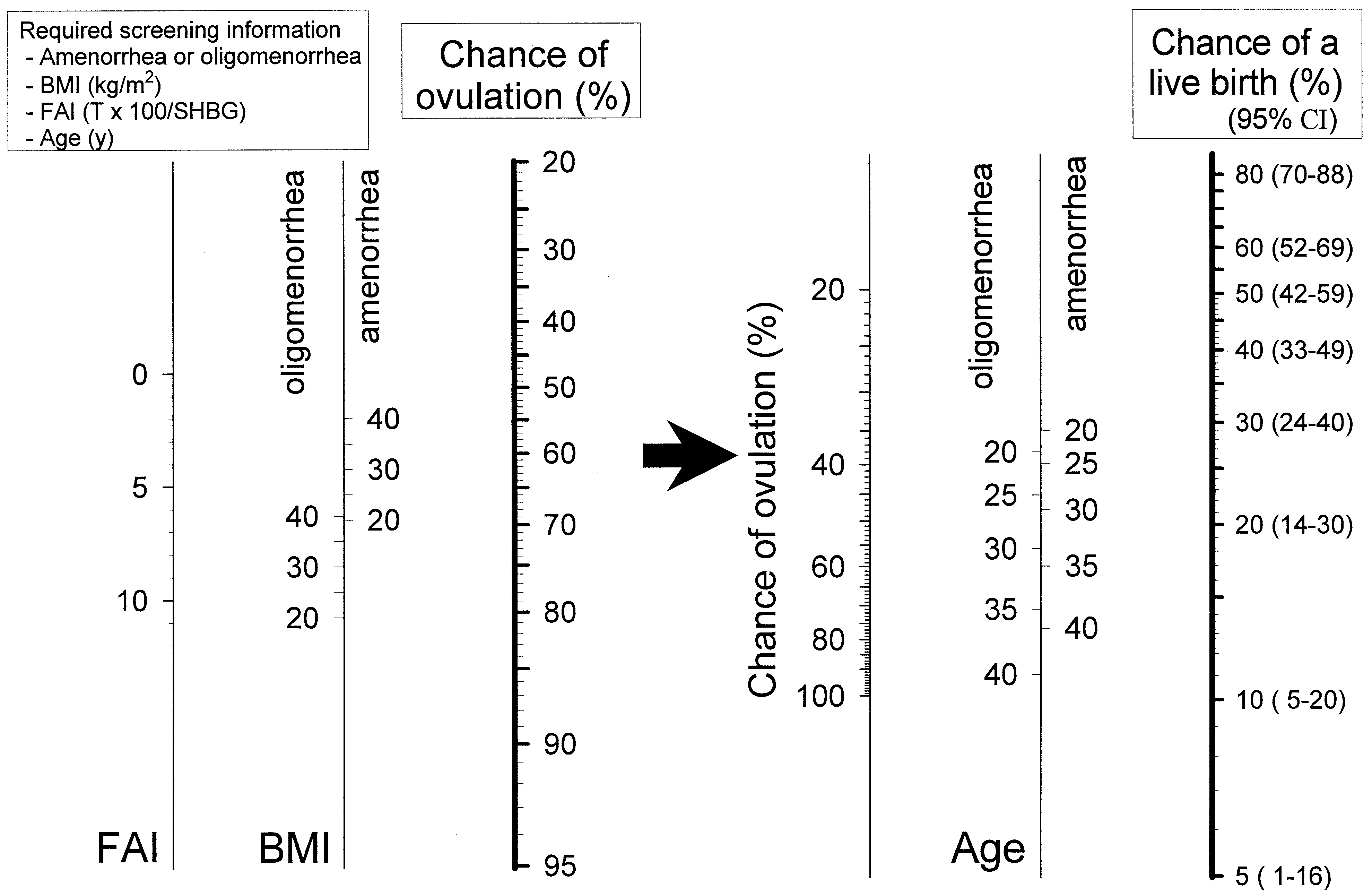
Figure 3 depicts the prediction of conception leading to
analyzed using the commercially available software package
live birth after CC treatment by applying a nomogram. This
nomogram comprises two separate steps. In the left panel,the probability of ovulation after CC administration can beestimated by applying FAI, BMI, and cycle history (oligo-
menorrhea versus amenorrhea). The chance to ovulate after
From the total of 259 patients fulfilling the inclusion/
CC treatment can be dragged-and-dropped from the left to
exclusion criteria and treated with CC, 186 (72%) suffered
the right panel. The right panel indicates the predicted prob-
from primary infertility and 62 (24%) from amenorrhea. We
ability of conception within 6 months after initiation of CC
found that 110 patients (43%) were obese (BMI Ͼ 27), 160
medication resulting in live birth; it combines the probability
patients (62%) presented with an elevated free androgen
of ovulation after CC with the patient’s age and cycle history
index (FAI) (FAI Ͼ 4.5), and 100 patients (39%) with
(oligomenorrhea versus amenorrhea). Because mean ovarian
hyperandrogenemia (testosterone Ն 3.2 nmol/L and/or an-
volume and serum leptin levels comprise the least predictive
drostenedione Ն 16.3 nmol/L (15, 17)). In 195 patients
contribution to the model (3, 12), they were excluded from
(75%), polycystic ovaries (mean ovarian volume Ն 10.8 mL
and/or mean follicle number per ovary Ն 10) (14, 15) were
The P value for the chi-square goodness-of-fit test was
diagnosed. In 121 patients (47%), an elevated initial LH
.49, indicating no statistically significant lack of fit between
(LH Ն 7.0 IU/L) (15) serum level was found. Sixty-five
the observed and predicted probability of live birth within
patients (25%) remained anovulatory after CC medication,
the five groups (see also the Methods section; data not
despite the maximum CC dose (150 mg/day), and were
FERTILITY & STERILITY
Odds ratios (OR) of initial screening characteristics in relation to the occurrence of ovulation in the entire group ofnormogonadotropic oligoamenorrheic infertile women (n ϭ 194 of 259) or live birth in ovulatory women after CC(n ϭ 98 of 194).
Bleeding interval in case of oligomenorrheab,e
Hyperandrogenemia (elevated T and/or AD)b
a Characteristics predicting conception in ovulatory CC patients applying multivariate analysis as published previously (Imani et al, JCEM 1999). b Biological relevant characteristics for ovarian dysfunction or pregnancy prediction in normogonadotropic anovulation. c Characteristics predicting ovulation following CC applying multivariate analysis as published previously (Imani et al., JCEM 1998, 2000). d The oligomenorrheic patients are 4 times more likely (OR ϭ 4.34) to ovulate after CC compared with amenorrheic patients. However, the chance for a livebirth after CC is 23% less (OR ϭ 0.77) compared with amenorrheic patients. e Amenorrhea is reference category for the categories of bleeding interval in oligomenorrhea. f FAI ϭ T ϫ 100/SHBG. g Polycystic ovaries ϭ mean ovarian volume Ն 10.8 mL and/or mean follicle number per ovary Ն 10 (van Stanbrink et al. Fertil Steril 1997). Imani. Prediction outcome clomiphene induction. Fertil Steril 2002.DISCUSSION
longitudinal cohort study. For the first time we used ovula-tion and conception as separate end points, taking into ac-
Currently, CC represents the first line of treatment for all
count that a significant proportion of patients remain anovu-
patients with normogonadotropic anovulatory infertility. The
latory during CC medication. These women are not exposed
present study confirms that CC is safe and convenient with
to the chances of becoming pregnant. Univariate and multi-
limited chances for complications such as multiple preg-
variate analyses were performed in these two separate set-
nancy or ovarian hyperstimulation syndrome. However, only
tings. The first multivariate model— consisting of FAI, BMI,
38% of treated women may conceive after receiving CC and
cycle history, and mean ovarian volume—predicts the wom-
have a live birth, which is substantially fewer than is gen-
an’s chances of remaining anovulatory after CC administra-
erally assumed. It may represent a distinct step forward in
tion (3). The second model— consisting of age and cycle
assisted reproductive services if patients with even lowerchances for live birth after a CC protocol could be identified
history—predicts the chances for conception only in women
who respond to CC treatment (4). The observed screeningcharacteristics involved in the prediction of ovulation after
Previous attempts by retrospective studies that included
CC medication are distinctly different from the predictors of
the entire group of anovulatory patients failed to identify
conception in ovulatory CC patients.
factors predicting ovulation (6, 7, 9) or conception (6, 8, 11)after CC treatment. In contrast, we focused on predictors of
In the current study we combine both prediction models
CC treatment outcome in a prospective fashion in the current
in a nomogram to predict the chances of live birth in the
Imani et al.
Cumulative percentage of women reaching first ovulation
The impact of cycle history on cumulative ovulation (A) and
and first conception ending in a live birth in 259 normogona-
live birth (B) rates in 259 normogonadotropic oligoamenor-
dotropic oligoamenorrheic infertile patients treated with CC
rheic infertile patients treated with CC therapy. Solid line ϭ
therapy. Solid line ϭ first ovulation after CC administration
oligomenorrheic patients (n ϭ 197). PϽ.001. Dashed line ϭ
(n ϭ 194; 75%); dashed line ϭ first conception ending in a
amenorrheic patients (n ϭ 62). P ϭ not applicable in the
overall WHO 2 anovulatory patients. PϽ.001 in ovulatorypatients following CC therapy. P values represent differencesapplying log rank test. Imani. Prediction outcome clomiphene induction. Fertil Steril 2002.
entire group of normogonadotropic anovulatory patients. Be-cause of its applicability in clinical practice, we convertedour analysis to a monthly basis rather than using treatmentcycles and we used live birth rather than pregnancy as theoutcome. Estimating a patient’s chance of ovulating is acrucial step in evaluating the probability of conception re-sulting in live birth after CC therapy. This is the reason forthe involvement of two steps in the presented nomogram.
Cycle history is the only factor that is present in both
steps. Amenorrheic patients are less likely to ovulate afterCC medication; however, once they ovulate, their chancesfor live birth are higher compared with oligomenorrheicwomen. A biologically plausible explanation is that theoccurrence of other factors contributing to a reduced fertilityis less likely, because these women never had the chance toconceive. BMI does not influence live birth rate in patientswho ovulate following CC therapy. Moreover, the live birth
Imani. Prediction outcome clomiphene induction. Fertil Steril 2002.
rate for CC-ovulatory polycystic ovary patients versus CC-ovulatory nonpolycystic ovary patients are comparable. It isof interest that age does not affect chances for ovulation but
association between reduced treatment outcome after in vitro
is involved in pregnancy chances once ovulation has been
fertilization and a patient’s advanced age (18).
reached (3, 4). This is in agreement with reports of an
Our major aim was to render the present nomogram as
FERTILITY & STERILITY
The probability of ovulation and conception ending in a live birth within 6 months after initiation of CC therapy applying anomogram. Chances for ovulation following CC administration can be assessed using FAI, BMI, and cycle history (left panel). The probability of conception ending in a live birth within 6 months after initiation of CC therapy can be assessed by combiningthe probability to ovulate with the age and the cycle history of the woman (right panel). To use this nomogram, encircle thevalues related to each screening parameter. Connect the circles to observe the predicted probability to ovulate. Correspondthis probability from the left to the right panel, and connect it with the woman’s age (separately for oligomenorrhea oramenorrhea) to predict the chance of a live birth. For instance, a 29-year-old amenorrheic woman presented with the followingfindings: FAI ϭ 9.3, BMI ϭ 32. Her chance to conceive leading to a live birth within 6 months after initiation of CC medicationwill be 19% (chance to ovulate following CC therapy: 50%). Imani. Prediction outcome clomiphene induction. Fertil Steril 2002.
easy as possible to use in daily clinical practice. Therefore,
0.82). Therefore, serum testosterone and SHBG levels are
ovarian volume (which was included in the previous multi-
the only endocrine factors that should be assessed for the
variate model predicting ovulation (3)) has been excluded
present nomogram. Indeed, both obesity and hyperandrogen-
from the present nomogram. The additional predictive con-
emia are associated with polycystic ovary syndrome, which
tribution of this prognostic factor to the model was negligi-
is known to exhibit low chances for success during CC
ble (a decrease in the area under the receiver characteristic
ovulation induction. Remaining biological plausible factors
curve of the model to predict patients remaining anovulatory
involved in ovarian dysfunction in normogonadotropic
from 0.82 to 0.80 (3)). We also demonstrated previously that
anovulation such as LH (17), insulin/glucose ratios (20),
serum leptin concentrations (an endocrine marker associated
inhibin B (21), and free IGF-I (22) levels failed to predict
with obesity (19)) predict chances of remaining anovulatory
ovulation or conception and were therefore excluded from
after CC therapy (12). Leptin has also been excluded from
the present nomogram because this assay is not available inmost hospital laboratories. Instead, information for BMI can
In summary, the present study demonstrates for the first
be generated easily with only a minor decrease in the area
time that a nomogram can be developed on the basis of initial
under the curve of the prediction model (0.85 instead of
screening characteristics that can predict the chances of live
Imani et al.
birth after CC therapy for a given patient. An external
7. Shepard MK, Balmaceda JP, Leija CG. Relationship of weight to
successful induction of ovulation with clomiphene citrate. Fertil Steril
validation of the present nomogram is mandatory to define a
clear cut-off level in the chances for live birth after CC
8. Hammond MG, Halme JK, Talbert LM. Factors affecting the pregnancy
rate in clomiphene citrate induction of ovulation. Obstet Gynecol 1983;
therapy for decision-making in routine daily clinical prac-
tice. For instance, a cut-off level of 20% chance of having a
9. Polson DW, Kiddy DS, Mason HD, Franks S. Induction of ovulation
with clomiphene citrate in women with polycystic ovary syndrome: the
live birth (which comprises 19% of the overall WHO 2
difference between responders and nonresponders. Fertil Steril 1989;
anovulatory patients) could be chosen. These patients could
10. Opsahl MS, Robins ED, O’Connor DM, Scott RT, Fritz MA. Charac-
be advised to refrain from CC therapy and start with an
teristics of gonadotropin response, follicular development, and endo-
alternative first-line treatment modality, such as weight re-
metrial growth and maturation across consecutive cycles of clomiphenecitrate treatment. Fertil Steril 1996;66:533–9.
duction, exogenous gonadotropins, insulin-sensitizing hor-
11. Kousta E, White DM, Franks S. Modern use of clomiphene citrate in
mones, or in vitro fertilization, particularly in women who
induction of ovulation. Hum Reprod Update 1997;3:359 – 65.
are of advanced age. This would render CC ovulation induc-
12. Imani B, Eijkemans MJ, de Jong FH, Payne NN, Bouchard P, Giudice
LC, et al. Free androgen index and leptin are the most prominent
tion strategies more patient-tailored and could improve their
endocrine predictors of ovarian response during clomiphene citrate
induction of ovulation in normogonadotropic oligoamenorrheic infer-tility. J Clin Endocrinol Metab 2000;85:676 – 82.
13. van Santbrink EJ, Hop WC, van Dessel TJ, de Jong FH, Fauser BC.
Decremental follicle-stimulating hormone and dominant follicle devel-opment during the normal menstrual cycle. Fertil Steril 1995;64:37– 43.
14. Pache TD, Wladimiroff JW, Hop WC, Fauser BC. How to discriminate
between normal and polycystic ovaries: transvaginal US study. Radi-ology 1992;183:421–3.
15. van Santbrink EJ, Hop WC, Fauser BC. Classification of normogona-
Acknowledgments: The authors thank Prof. John Collins, Hamilton, Ontario,
dotropic infertility: polycystic ovaries diagnosed by ultrasound versus
Canada, for his critical comments; and Professor Linda Giudice (Stanford
endocrine characteristics of polycystic ovary syndrome. Fertil Steril
University), Dr. Najiba Lahlou (Paris), and Professor Frank de Jong (Rot-
16. Kaplan EL, Meier P. Nonparametric estimation from incomplete ob-
servations. J Am Statist Assoc 1958;53:457– 81.
17. Fauser BC, Pache TD, Lamberts SW, Hop WC, de Jong FH, Dahl KD.
Serum bioactive and immunoreactive luteinizing hormone and follicle-
References
stimulating hormone levels in women with cycle abnormalities, with or
1. Greenblatt RB, Barfield WE, Jungck EC, Ray AW. Induction of ovu-
without polycystic ovarian disease. J Clin Endocrinol Metab 1991;73:
lation with MRL/41. JAMA 1961;178:127–30.
2. Rowe Pj, Comhaire FH, Hargreave TB, Mellows HJ, editors. WHO
18. Scott RT, Opsahl MS, Leonardi MR, Neall GS, Illions EH, Navot D.
manual for the standardized investigation and diagnosis of the infertile
Life table analysis of pregnancy rates in a general infertility population
couple. Cambridge: The Press Syndicate of the University of Cam-
relative to ovarian reserve and patient age. Hum Reprod 1995;10:1706 –
3. Imani B, Eijkemans MJ, te Velde ER, Habbema JD, Fauser BC.
19. Rouru J, Anttila L, Koskinen P, Penttila TA, Irjala K, Huupponen R, et
Predictors of patients remaining anovulatory during clomiphene citrate
al. Serum leptin concentrations in women with polycystic ovary syn-
induction of ovulation in normogonadotropic oligoamenorrheic infer-
drome. J Clin Endocrinol Metab 1997;82:1697–700.
tility. J Clin Endocrinol Metab 1998;83:2361–5.
20. Poretsky L, Cataldo NA, Rosenwaks Z, Giudice LC. The insulin-related
4. Imani B, Eijkemans MJ, te Velde ER, Habbema JD, Fauser BC.
ovarian regulatory system in health and disease. Endocr Rev 1999;20:
Predictors of chances to conceive in ovulatory patients during clomi-
phene citrate induction of ovulation in normogonadotropic oligoamen-
21. Anderson RA, Groome NP, Baird DT. Inhibin A and inhibin B in
orrheic infertility. J Clin Endocrinol Metab 1999;84:1617–22.
women with polycystic ovarian syndrome during treatment with FSH to
5. MacGregor AH, Johnson JE, Bunde CA. Further clinical experience
induce mono-ovulation. Clin Endocrinol (Oxf) 1998;48:577– 84.
with clomiphene citrate. Fertil Steril 1968;19:616 –22.
22. van Dessel HJ, Lee PD, Faessen G, Fauser BC, Giudice LC. Elevated
6. Gorlitsky GA, Kase NG, Speroff L. Ovulation and pregnancy rates with
serum levels of free insulin-like growth factor-1 (IGF-1) in polycystic
clomiphene citrate. Obstet Gynecol 1978;51:265–9.
ovary syndrome. J Clin Endocrinol Metab 1999;84:3030 –5. FERTILITY & STERILITY
2013-2014 THAYER ACADEMY _______________________ lth Services Medical Consent for Student To Be Completed by PARENT/GUARDIAN (Please print clearly in ink .) Student Cel # : (______)_____________________ CONTACT INFORMATION Student Email : ________________________@_______________________ Student Name LAST : __________________________________ FIRST
For Immediate Release Media Contacts Britni Manry 469-619-7156 bmanry@uplifteducation.org Kelly Lane Kelly.Lane@LevensonBrinkerPR.com 214-351-1586 Uplift Education charter school helps move economically disadvantaged students in West Dallas to the top of the class Heights Preparatory rated “Exemplary” school in first year of operation DALLAS (August 8, 2011) –
 Odds ratios (OR) of initial screening characteristics in relation to the occurrence of ovulation in the entire group ofnormogonadotropic oligoamenorrheic infertile women (n ϭ 194 of 259) or live birth in ovulatory women after CC(n ϭ 98 of 194).
Odds ratios (OR) of initial screening characteristics in relation to the occurrence of ovulation in the entire group ofnormogonadotropic oligoamenorrheic infertile women (n ϭ 194 of 259) or live birth in ovulatory women after CC(n ϭ 98 of 194).

 Cumulative percentage of women reaching first ovulation
The impact of cycle history on cumulative ovulation (A) and
Cumulative percentage of women reaching first ovulation
The impact of cycle history on cumulative ovulation (A) and
 The probability of ovulation and conception ending in a live birth within 6 months after initiation of CC therapy applying anomogram. Chances for ovulation following CC administration can be assessed using FAI, BMI, and cycle history (left panel).
The probability of ovulation and conception ending in a live birth within 6 months after initiation of CC therapy applying anomogram. Chances for ovulation following CC administration can be assessed using FAI, BMI, and cycle history (left panel).