An extract of black, green, and mulberry teas causes malabsorptionof carbohydrate but not of triacylglycerol in healthy volunteers1–3
Litao Zhong, Julie K Furne, and Michael D LevittABSTRACT
in green tea are dimerized to form a variety of theaflavins (1);
Background: In vitro studies suggest that extracts of black, green,
thus, these teas may have different biological activities.
and mulberry teas could interfere with carbohydrate and triacylglyc-
A putative beneficial effect of tea is its ability to induce weight
erol absorption via their ability to inhibit ␣-amylase, ␣-glucosidase,
loss. Support for this contention includes a controlled human trial
sodium-glucose transporters, and pancreatic lipase.
that showed weight loss when tea was added to a dietary regimen
Objective: We measured breath hydrogen and 13CO to investigate
(2) and a mouse study that showed that administration of a tea
the ability of an extract of black, green, and mulberry tea leaves to
extract with a high-fat diet eliminated the weight gain observed
induce malabsorption of carbohydrate and triacylglycerol in healthy
in the absence of tea (3). Several mechanisms have been postu-
lated to account for this weight control. Modest increases in
Design: In a crossover design, healthy adult volunteers randomly
energy expenditure have been reported with the ingestion of
ingested test meals with a placebo beverage or a preparation con-
oolong and green teas (4 – 6). In addition, tea could inhibit the
taining an extract of black (0.1 g), green (0.1 g), and mulberry (1.0
absorption of carbohydrate or fat. In vitro experiments have
g) teas. One test meal contained 50 g carbohydrate as white rice, 10 g
shown that constituents of tea inhibit the activities of ␣-amylase
butter, and 0.2 g [13C]triolein, and the beverages contained 10 g
(7–10) and ␣-glucosidase (11–16) and of intestinal sodium-
sucrose. The calorie content of the second test meal consisted en-
dependent glucose transporters (17–21). The in vitro inhibition
tirely of lipid (30 g olive oil and 0.2 g [13C]triolein). Breath-
of pancreatic lipase (22–24) by tea extracts suggests that tea
hydrogen and 13CO concentrations were assessed hourly for 8 h,
might interfere with triacylglycerol absorption. However, no in
and symptoms were rated on a linear scale.
vivo studies in humans or animals have shown that tea prepara-
Results: With the carbohydrate-containing meal, the tea extract
tions cause malabsorption of carbohydrate or fat. In the present
resulted in a highly significant increase in breath-hydrogen concen-
report, we measured breath hydrogen and 13CO to investigate
trations, which indicated appreciable carbohydrate malabsorption.
the ability of an extract of black, green, and mulberry tea leaves
A comparison of hydrogen excretion after the carbohydrate-
to induce malabsorption of carbohydrate and triacylglycerol in
containing meal with that after the nonabsorbable disaccharide lac-
tulose suggested that the tea extract induced malabsorption of 25%of the carbohydrate. The tea extract did not cause triacylglycerolmalabsorption or any significant increase in symptoms. SUBJECTS AND METHODS Conclusion: This study provides the basis for additional experi-
The study was approved by the Human Studies Subcommittee
ments to determine whether the tea extract has clinical utility for the
of the Minneapolis Veterans Affairs Medical Center, and in-
formed consent was obtained from all subjects. Study A: carbohydrate- and lipid-containing test meal KEY WORDS
Malabsorption, carbohydrate, triacylglycerol,
Twenty healthy volunteers (10 women and 10 men) aged
tea extract, breath-hydrogen test, 13CO -breath test
23– 60 y fasted after their usual dinner until the following morn-ing (Ȃ0800), when the experiments were performed at the Min-neapolis Veterans Affairs Medical Center. After collection of
INTRODUCTION
baseline breath samples for hydrogen and 13CO analysis, the
It is widely believed that teas contain substances that are ben-
subjects ingested a test meal consisting of white rice and butter.
eficial to health. (A search of the key words “tea health benefits”brings up 5 million entries on Google.) Although most of the
1 From NatureGen Inc, San Diego, CA (LZ), and VAMC (Research Ser-
alleged benefits of tea are not supported by solid scientific evi-
vice/151), Minneapolis, MN (JKF and MDL).
dence, teas contain a variety of biologically active compounds
Supported by NatureGen, Inc, San Diego, CA, and VAMC (Research
that might influence metabolic reactions. Most of the commonly
3 Reprints not available. Address correspondence to MD Levitt, VAMC
ingested teas are derived from the leaf of the Camellia sinensis
(Research Service/151), 1 Veterans Drive, Minneapolis, MN 55417. E-mail:
plant, and various types of tea are created via manipulations (eg,
drying, fermentation) of this leaf. As green tea is fermented to
oolong and then to black tea, polyphenol compounds (catechins)
Accepted for publication April 29, 2006. Am J Clin Nutr 2006;84:551–5. Printed in USA. 2006 American Society for Nutrition
The rice was boiled for 20 min, and then individual portions (176g containing 50 g carbohydrate) were frozen with 10 g butter. Immediately before being ingested, the meals were warmed in amicrowave oven, and 0.2 g [13C]triolein (Cambridge IsotopeLaboratories, Andover, MA) was thoroughly mixed into themeal. Five hundred milliliters warm water and 10 g sucrose wereadded to the tea extract beverage or placebo preparation, whichwere well stirred. The subjects were randomly assigned to drinkeither the tea extract or the placebo beverage concurrently withthe meal. Breath samples were then collected at hourly intervalsfor 8 h. At the end of each test period, the subjects were asked torate a variety of symptoms—including nausea, bloating, abdom-inal discomfort, rectal gas, and obfuscating symptoms— on apreviously described linear scale that ranged from 0 (none) to 4(severe) (25). In addition, loose bowel movements were noted. FIGURE 1. Mean (ȀSEM) breath-hydrogen concentrations in 20 sub-
One week later the test was repeated after the subjects ingested
jects who ingested a meal consisting of 50 g rice (carbohydrate), 10 g butter,and 0.2 g [13C]triolein with a tea extract beverage (ᮀ) or a placebo beverage
the opposite preparation from that ingested in the initial study.
(F), both of which contained 10 g sucrose. The significance of the differenceswas determined with a 2-tailed paired t test. Values obtained with the 2
Study B: lipid-containing, carbohydrate-free test meal
treatments were not significantly different between the 0- and 1-h measure-ments. Each hourly measurement from 2 to 8 h, however, was significantly
Ten of the subjects took part in a second study that followed the
greater when the tea extract was ingested (P ҃ 0.026 at 2 h, P ҃ 0.013 at 3 h,
same format as study A; however, the caloric content of the meal
and P 0.003 from 4 to 8 h).
consisted entirely of lipid (30 g olive oil plus 0.2 g [13C]triolein). The tea leaf extract or placebo was similar to that described in theprevious study; however, sucrose was replaced with 1 g of the
each breath sample relative to that of the baseline sample was
noncaloric sweetener sucralose (Splenda McNeil Nutritionals,
determined by mass spectroscopy, which was performed by a
Fort Washington, PA). Breath samples were obtained for 13CO
commercial laboratory (Metabolic Solutions Inc, Nashua, NH).
measurements as described in study A. Statistics and calculations Test products
The significance of differences between means observed with
the 2 treatments was determined by 2-tailed paired t test. The
The active preparation, a proprietary product, consisted of a
quantity of carbohydrate malabsorption induced by the tea ex-
mixture of extracts of green (0.1 g), black (0.1 g), and mulberry
tract preparation was estimated by first determining the differ-
(1.0 g) tea leaves. The approximate quantities of the potential
ence between the sum of breath-hydrogen concentrations ob-
antiabsorptive components per dose of our tea extract beverage
served over hours 1– 8 when subjects ingested tea extract or
(measured by HPLC) were as follows: 5 mg deoxynojirimycin-
placebo. The grams of carbohydrate represented by this differ-
type compounds, 100 mg epicatechin gallate, 300 mg epigallo-
ence in hydrogen were estimated by comparison with the previ-
catechin gallate, and 100 mg theaflavin. The control beverage
ously observed difference in the sum of hydrogen concentrations
contained trace quantities of red dye no. 40 and caramel to pro-
over hours 1– 8 when 55 healthy subjects ingested 10 g lactulose
vide a brown color similar to that of the tea extract. (Both prod-
or a noncaloric beverage (27). The excess sum of breath-
ucts were supplied by NatureGen Inc, San Diego, CA.) The taste
hydrogen concentrations observed with 10 g lactulose averaged
of the 2 test materials differed, and subjects were aware of the
6.2 mol/L; thus, carbohydrate malabsorption induced by tea
extract in the present study was estimated from the formula
Breath collections
Expired air was sampled for hydrogen concentration as de-
scribed previously (26). Breath samples for 13CO analysis were
collected by having the subject expire through a straw into a glass
tube (Labco Exetainer; Labco International Inc, Houston, TX),which was sealed immediately after withdrawal of the straw. Analyses
Each breath collection for hydrogen measurement was ana-
Breath-hydrogen concentration
lyzed for carbon dioxide (Capstar 100; CWE Inc, Ardmore, PA)
The mean (ȀSEM) hourly breath-hydrogen concentrations
to ensure that an adequate alveolar sample had been collected.
observed after ingestion of the rice and butter meal with each of
The hydrogen concentration of the rare sample that contained
the 2 treatments are shown in Figure 1. The hydrogen concen-
4.5% CO (5 of 360 samples) was normalized to 5% CO
tration at baseline was not significantly different from that at 1 h.
(observed hydrogen concentration ҂ 5%/observed carbon diox-
However, the curves significantly diverged by 2 h, with the
ide concentration). The hydrogen concentration was measured
breath-hydrogen concentration being significantly greater in the
by gas chromatography with a molecular sieve column, nitrogen
group receiving the tea extract beverage at each hourly time point
as the carrier gas, and a reduction detector (Trace Analytic,
from 2 to 8 h. The sum of the breath-hydrogen concentrations for
Menlo Park, CA). The atom percent (atom%) excess of 13CO in
hours 1– 8 (a value that closely approximated the area under the
TEA EXTRACT INDUCES MALABSORPTION OF CARBOHDYRATE
TABLE 1 Comparison of symptoms reported by healthy subjects in the 8-h period after ingestion of a standard carbohydrate- and lipid-containing meal plus a tea extract or placebo 1 Symptoms were rated on a linear scale of 0 (none) to 4 (severe). 2 Calculated with a 2-tailed paired t tests, not corrected for multiple
3 x Ȁ SEM (all such values). Symptoms
The severity of symptoms reported by the subject for the 8 h of
study A are shown in Table 1. No significant differences (P FIGURE 2. Mean (ȀSEM) atom% excess of 13C in expired air after
0.05) in symptoms were observed for any symptom between the
ingestion of 2 different test meals: a tea extract (ᮀ) or a placebo (F). The
2 treatment groups. Similarly, no significant differences in symp-
significance of the differences was determined with a 2-tailed paired t test.
toms were observed between the 2 treatment groups in study B
Study A: results for 20 healthy subjects who ingested a meal consisting of 50 g
carbohydrate as rice, 10 g butter, and 0.2 g [13C]triolein with the tea extractor placebo solution, both of which contained 10 g sucrose. Values at 0 – 4 hwere not significantly different between the 2 treatment groups. The valueswere significantly greater in the tea extract group than in the placebo group
DISCUSSION
at 5– 8 h (P ҃ 0.014 at 5 h and P 0.001 at 6 – 8 h). Study B: results for 10
We used measurements of breath-hydrogen and of breath-
subjects who ingested a carbohydrate-free meal consisting of 30 g olive oil
and 0.2 g [13C]triolein with the tea extract or placebo solution, both of which
CO to determine whether ingestion of a tea extract preparation
contained 1 g sucralose (noncaloric sweetener). No significant differences
induced malabsorption of carbohydrate or fat. Carbohydrate
were observed at any time point (P 0.2).
malabsorption provides substrate for most of the hydrogen pro-duced in humans, which can be assessed by measuring breath-
curve for 1– 8 h) averaged 12.2 Ȁ 2.0 and 2.7 Ȁ 0.6 mol/L in the
hydrogen concentrations (28, 29). In contrast, fat is not fer-
groups receiving tea extract and placebo, respectively (P
mented to carbon dioxide by the colonic bacteria, and carbon
0.001). Using Equation 1, this difference in hydrogen (9.5
dioxide production from lipid reflects the host’s metabolism of
mol/L) indicated that the tea extract induced malabsorption of
absorbed lipid. Studies using triolein labeled with 13C (30, 31) or
Ȃ15 g of the 60 g of carbohydrate in the meal over the 8-h test
14C (32, 33) showed that fat malabsorption documented by fecal
fat measurements was associated with a reduction in labeledcarbon dioxide excretion. Breath-13CO measurements
In the present study, the subjects ingested standard meals with
The mean (ȀSEM) hourly 13C atom% excesses (hourly values
a beverage containing tea extract or placebo. The initial test meal
minus baseline value) for the 2 treatments when subjects ingested
contained 60 g carbohydrate (50 g starch as white rice and 10 g
the rice and butter meal (study A) are shown in Figure 2. Al-
sucrose in the tea extract or the placebo) and 10.2 g fat. White rice
though the measurements at hours 1– 4 were not significantly
was used as the complex carbohydrate because, in contrast with
different between the 2 treatments, the values were significantly
most complex carbohydrates, rice starch is nearly completely
higher for tea extract than for placebo at hours 5– 8. The sum
absorbed by healthy subjects (34). Thus, a rice meal allows
of the values for hours 1– 8 averaged 0.0256 Ȁ 0.0017 and
breath testing to more sensitively determine whether a manipu-
0.0213 Ȁ 0.0019 atom% excess for the tea extract and the
lation significantly increases hydrogen excretion, ie, causes
placebo, respectively (P ҃ 0.014). The 13C atom% excess
starch malabsorption. As shown in Figure 1, the breath-hydrogen
values after ingestion of the lipid-containing (30 g olive oil plus
concentration declined with the placebo, which indicated that
[13C]triolein), carbohydrate-free meal (study B) are shown in
residual fermentable colonic substrate was not replenished via
Figure 2. In contrast with the results in study A, the sum of the
malabsorption of carbohydrate in the test meal. In contrast, the
values for hours 1– 8 for the tea extract (0.012 Ȁ 0.0025 atom%
ingestion of tea extract resulted in increased breath-hydrogen
excess) was virtually identical to that with the placebo (0.012 Ȁ
concentrations, which were significantly greater than the values
0.0023 atom% excess) (P ҃ 0.95), and none of the hourly mea-
observed with placebo for each hourly measurement between 2
surements showed significant differences (P 0.2) between the
and 8 h. Thus, the tea extract clearly induced malabsorption of the
The carbohydrate malabsorption induced by the tea extract
indicates that carbohydrate malabsorption induced by tea ex-
was estimated by comparing the difference in breath-hydrogen
tracts also could influence blood glucose concentrations. A sim-
concentrations between the tea extract and placebo groups with
ilar observation has been reported with an extract of the root of
those observed previously (27) in healthy volunteers who in-
Salacia oblonga (44, 45). This extract reduces glucose absorp-
gested 10 g lactulose (see Equation 1). This calculation suggested
tion via inhibition of intestinal ␣-glucosidase by 2 compounds,
that Ȃ15 g of the 60 g of carbohydrate in the test meal was not
salcinol and kotanol, that differ in structure from the
absorbed. This may be a low estimate because nonabsorbed ma-
␣-glucosidase inhibitors in the tea preparation. It also should be
terial in the test meal could have been fermented less rapidly than
noted that 2 ␣-glucosidase–inhibiting drugs of bacterial origin
(acarbose and miglitol) are available for the treatment of diabe-
Elucidation of the mechanisms and specific tea extracts re-
tes. However, the use of these drugs in the United States has been
sponsible for the carbohydrate malabsorption will require addi-
limited by side effects (eg, gas and diarrhea) and by a relatively
tional studies. Mulberry leaf contains alkaloids of the
minor effect on blood glucose concentrations. The structure of
1-deoxynojirimycin type that inhibit intestinal ␣-glucosidase
␣-glucosidase inhibitors in mulberry tea differs from that of
(14). Green tea supplies epicatechin gallate and epigallocatechin
acarbose, but is similar to that of miglitol. It remains to be de-
gallate, compounds that inhibit mucosal sodium-glucose trans-
termined whether carbohydrate malabsorption induced by our
porters (17, 18). Black tea, via its theaflavin content, is an inhib-
tea extract offers any benefits over those obtained with acarbose
itor of ␣-amylase (8). The quantities of these compounds in one
or miglitol. Although a significant increase in gaseous symptoms
dose of our tea extract preparation are equivalent (depending on
was not reported after ingestion of either the tea extract or the
the compound) to that which would be contained in 5–20 cups
placebo (Table 1), studies in which tea extract is administered
(1.2– 4.8 L) of conventional tea. The extraction process reduced
with each meal should be performed before it can be claimed that
the caffeine of the tea extract to 50% of that of 1 cup (0.24 L) of
tea extract–induced carbohydrate malabsorption is associated
with fewer symptoms than has been observed with ␣-glucosi-
dase–inhibiting drugs. Indeed, it would be surprising if the de-
CO measurements did not support the concept that
gree of malabsorption observed with the tea extract (25% of total
the tea extract inhibited triacylglycerol absorption. Rather, the13
ingested carbohydrate) were not associated with some degree of
CO concentration was significantly greater when tea extract
accompanied the standard meal (Figure 2), a finding that cannot
Extracts of black, green, and mulberry teas have been con-
be explained by tea extract enhancing the absorption of lipid
sumed for many years by enormous numbers of Asians, and
because [13C]triolein absorption should approach 100% with the
these products are considered safe. Green and black tea ex-
placebo. One possible explanation is that the extract-induced
tracts also are widely used in the Western world. Although tea
carbohydrate malabsorption resulted in more rapid oxidization
extracts have been shown to interact with the metabolism of
of newly absorbed, labeled lipid because of the lesser availability
other drugs (46, 47), serious complications possibly attribut-
of glucose for energy utilization. It is also possible that the tea
able to ingestion of these extracts are rare (48). Thus, although
extract caused more rapid oxidation of absorbed [13C]oleic acid,
the potential for unintended serious side effects is seemingly
independent of differences in carbohydrate absorption (4). To
low, rare unexpected side effects of the extract can be confi-
differentiate between these 2 possibilities, 10 subjects ingested a
dently excluded only after the product has been consumed in
lipid-containing (30 g olive oil containing [13C]triolein),
an environment where medical surveillance is adequate to
carbohydrate-free meal plus the tea extract or placebo. No sig-
nificant differences in 13CO excretion were observed, which
suggested that the higher 13CO noted with the carbohydrate-
JKF helped design the protocol, recruited the subjects, and analyzed the
containing meal reflected the influence of the extract-induced
data. MDL contributed to the design of the protocol, analyzed the data, and
carbohydrate malabsorption on lipid metabolism.
wrote the manuscript. LZ was involved in the design of the protocol but hadno involvement in the collection or analysis of the data. LZ is president of
The ability of a tea extract to inhibit carbohydrate absorption
NatureGen, the company that provided the tea extract and placebo used in this
has potential clinical utility for weight control and the treatment
study. JKF and MDL had no financial interest in NatureGen or any other type
of diabetes. Assuming that the tea extract causes malabsorption
of conflict of interest with the material presented in this article.
of 25% of ingested carbohydrate, striking weight loss would beexpected providing that caloric intake was not commensuratelyincreased and the caloric content of malabsorbed carbohydratewas unavailable to the host. Malabsorption of 25% of 400 g
REFERENCES
1. Leung LK, Su Y, Chen R, Zhang Z, Huang Y, Chen ZY. Theaflavins in
carbohydrate/d would reduce the caloric availability by
black tea and catechins in green tea are equally effective antioxidants. J
Ȃ146 000 calories (16 kg fat) per year. Although it is commonly
assumed that the host obtains no calories from materials entering
2. Nagao T, Komine Y, Soga S, et al. Ingestion of a tea rich in catechins
the colon, the colonic absorption of carbohydrate fermentation
leads to a reduction in body fat and malondialdehyde-modified LDL in
products results in an appreciable conservation of calories (36).
men. Am J Clin Nutr 2005;81:122–9.
3. Han LK, Takaku T, Li J, Kimura Y, Okuda H. Anti-obesity action of
Thus, weight loss would be less than the predicted 16 kg/y.
oolong tea. Int J Obes Relat Metab Disord 1999;23:98 –105.
For centuries, teas have been used as a treatment for diabetes
4. Rumpler W, Seale J, Clevidence B, et al. Oolong tea increases metabolic
mellitus in Asia. Multiple studies have shown that extracts of
rate and fat oxidation in men. J Nutr 2001;131:2848 –52.
mulberry and other teas reduce blood glucose in type 2 diabetic
5. Dulloo AG, Duret C, Rohrer D, et al. Efficacy of a green tea extract rich
in catechin polyphenols and caffeine in increasing 24-h energy expen-
persons (37–39) and in animal models of diabetes (40 – 43). This
diture and fat oxidation in humans. Am J Clin Nutr 1999;70:1040 –5.
hypoglycemic effect generally has been attributed to alterations
6. Berube-Parent S, Pelletier C, Dore J, Tremblay A. Effects of encapsu-
of the intermediary metabolism of glucose. The present study
lated green tea and Guarana extracts containing a mixture of
TEA EXTRACT INDUCES MALABSORPTION OF CARBOHDYRATE
epigallocatechin-3-gallate and caffeine on 24 h energy expenditure and
28. Levitt MD. Production and excretion of hydrogen gas in man. N Engl
fat oxidation in men. Br J Nutr 2005;94:432– 6.
7. Kashket S, Paolino VJ. Inhibition of salivary amylase by water-soluble
29. Levitt MD, Donaldson RM. Use of respiratory hydrogen excretion to
extracts of tea. Arch Oral Biol 1988;33:845– 6.
detect carbohydrate malabsorption. J Lab Clin Med 1970;75:937– 45.
8. Zhang J, Kashket S. Inhibition of salivary amylase by black and green
30. Amarri S, Harding M, Coward WA, Evans TJ, Weaver LT. 13C and H2
teas and their effects on the intraoral hydrolysis of starch. Caries Res
breath tests to study extent and site of starch digestion in children with
cystic fibrosis. J Pediatr Gastroenterol Nutr 1999;29:327–31.
9. Hansawasdi C, Kawabata J, Kasai T. Alpha-amylase inhibitors from
31. Amarri S, Harding M, Coward WA, Evans TJ, Weaver LT. 13Carbon
roselle (Hibiscus sabdariffa Linn. ) tea. Biosci Biotechnol Biochem
mixed triglyceride breath test and pancreatic enzyme supplementation in
cystic fibrosis. Arch Dis Child 1997;76:349 –51.
10. Funke I, Melzig MF. Effect of different phenolic compounds on alpha-
32. Newcomer AD, Hofmann AF, DiMagno EP, Thomas PJ, Carlson GL.
amylase activity: screening by microplate-reader based kinetic assay.
Triolein breath test: a sensitive and specific test for fat malabsorption.
11. Oki T, Matsui T, Matsumoto K. Evaluation of alpha-glucosidase inhi-
33. Einarsson K, Bjorkhem I, Eklof R, Blomstrand R. 14-C triolein breath test
bition by using an immobilized assay system. Biol Pharm Bull 2000;23:
as a rapid and convenient screening test for fat malabsorption. Scand J
12. Matsui T, Yoshimoto C, Osajima K, Oki T, Osajima Y. In vitro survey
34. Levitt MD, Hersh P, Fetzer CA, Sheahan M, Levine AS. H excretion
of alpha-glucosidase inhibitory food components. Biosci Biotechnol
after ingestion of complex carbohydrates. Gastroenterology 1987;92:
13. Watanabe J, Kawabata J, Kurihara H, Niki R. Isolation and identification
35. Christl SU, Murgatroyd PR, Gibson GR, Cummings JH. Quantitative
of alpha-glucosidase inhibitors from tochu-cha (Eucommia ulmoides).
measurement of hydrogen and methane from fermentation using a whole
Biosci Biotechnol Biochem 1997;61:177– 8.
body calorimeter. Gastroenterology 1992;102:1269 –77.
14. Asano N, Oseki K, Tomioka E, Kizu H, Matsui K. N-containing sugars
36. Bond JH, Levitt MD. Fate of soluble carbohydrate in the colon of rats and
from Morus alba and their glycosidase inhibitory activities. Carbohydr
man. J Clin Invest 1976;57:1158 – 64.
37. Andallu B, Suryakantham V, Srikanthi BL, Reddy KS. Effect of mul-
15. Miyahara C, Miyazawa M, Satoh S, Sakai A, Mizusaki S. Inhibitory
berry (Morus Indica L.) therapy on plasma and erythrocyte membrane
effects of mulberry leaf extract on postprandial hyperglycemia in normal
lipids and patients with type 2 dibetes. Clin Chim Acta 2001;314:47–53.
rats. J Nutr Sci Vitaminol (Tokyo) 2004;50:161– 4.
38. Hosoda K, Wang MF, Liao ML, et al. Anti hyperglycemic effect of
16. Asano N, Yamashita T, Yasuda K, et al. Polyhydroxylated alkaloids
oolong tea in type 2 dibetes. Diabetes Care 2003;26:714 – 8.
isolated from mulberry trees (Morusalba L.) and silkworms (Bombyx
39. Jayawardena MH, deAlwis NM, Hettigoda V, Ferando DJ. A double
mori L.). J Agric Food Chem 2001;49:4208 –13.
blind randomised placebo controlled cross over study of a herbal prep-
17. Kobayashi Y, Suzuki M, Satsu H, et al. Green tea polyphenols inhibit the
aration containing Salacia reticulata in the treatment of type 2 diabetes.
sodium-dependent glucose transporter of intestinal epithelial cells by a
competitive mechanism. J Agric Food Chem 2000;48:5618 –23.
18. Shimizu M, Kobayashi Y, Suzuki M, Satsu H, Miyamoto Y. Regulation
40. Clark TA, Edel AL, Heyliger CE, Pierce GN. Effective control of gly-
of intestinal glucose transport by tea catechins. Biofactors 2000;13:
cemic status and toxicity in Zucker diabetic fatty rats with an orally
administered vanadate compound. Can J Physiol Pharmacol 2004;82:
19. Kreydiyyeh SI, Abdel-Hasan Baydoun E, Churukian ZM. Tea extract
inhibits intestinal absorption of glucose and sodium in rats. Comp Bio-
41. Gomes A, Vedasiromoni JR, Das M, Sharma RM, Ganguly DK. Anti-
chem Physiol C Pharmacol Toxicol Endocrinol 1994;108:359 – 65.
hyperglycemic effect of black tea (Camellia sinensis) in rat. J Ethno
20. Gurman EG, Bagirova EA, Storchilo OV. The effect of food and drug
herbal extracts on the hydrolysis and transport of sugars in the rat small
42. Shenoy C. Hypoglycemic activity of bio-tea in mice. Indian J Exp Biol
intestine under different experimental conditions. Fiziol Zh SSSR Im I M
43. Tsuneki H, Ishizuka M, Terasawa M, Wu JB, Sasaoka T, Kimura I.
21. Shimizu M. Modulation of intestinal functions by food substances.
Effect of green tea on blood glucose levels and serum proteomic patterns
in diabetic (db/db) mice and on glucose metabolism in healthy humans.
22. Juhul C, Armand N, Pafumi Y, Rosier C, Vandermander J, Lairon D.
Green tea extract (AR25) inhibits lipolysis of triglycerides in gastric and
44. Collene AL, Hertzler SR, Williams JA, Wolf BW. Effects of a nutritional
duodenal medium in vitro. J Nutr Biochem 2000;11:45–51.
supplement containing Salacia oblonga extract and insulinogenic amino
23. Nakai M, Fukui Y, Asami S, et al. Inhibitory effects of oolong tea
acids on postprandial glycemia, insulinemia and breath hydrogen re-
polyphenols on pancreatic lipase in vitro. J Agric Food Chem 2005;53:
sponses in healthy adults. Nutr 2005;21:848 –54.
45. Heacock PM, Hertzler SR, Williams JA, Wolf BW. Effects of a medical
24. Han L-K, Kimura Y, Kawashima M, et al. Anti-obesity effects in rodents
food containing an herbal ␣-glucosidase inhibitor on postprandial gly-
of dietary tea saponin, a lipase inhibitor. Int J Obes Relat Metab Disord
cemia and insulinemia in healthy adults. J Am Diet Assoc 2005;105:65–
25. Suarez FL, Zumarraga LM, Furne JK, Levitt MD. Nutritional supple-
46. Nishikawa M, Ariyoshi N, Kotani A, et al. Effects of continuous inges-
ments used in weight reduction programs increase intestinal gas in per-
tion of green tea or grape seed extracts on the pharmacokinetics of
sons who malabsorb lactose. J Am Diet Assoc 2001;101:1447–52.
midazolam. Drug Metab Pharmacokinet 2004;19:280 –9.
26. Suarez FL, Savaiano DA, Levitt MD. A comparison of symptoms with
47. Jang EH, Choi JY, Park CS, et al. Effects of green tea extract adminis-
milk or lactose-hydrolyzed milk in people with self-reported severe
tration on the pharmacokinetics of clozapine in rats. J Pharm Pharmacol
lactose intolerance. N Engl J Med 1995;333:1– 4.
27. Strocchi A, Corazza G, Ellis CJ, Gasbarrini G, Levitt MD. Detection of
48. Gloro R, Hourmand-Ollivier I, Mosquet B, et al. Fulminant hepatitis
malabsorption of low doses of carbohydrate: accuracy of various breath
during self-medication with hydroalcoholic extract of green tea. Eur J
H criteria. Gastroenterology 1993;105:1404 –10.
Gastroenterol Hepatol 2005;17:1135–7.
working down. Use progressively closer settings to get the “look” and LITHIUM ION TRIMMER Instructions 2. For hard to reach or tight areas, use the detailer head. Always pull skin taut. Then slowly move the detailer through area to trim until TRIMMING AND EDGING YOUR BEARD The following are suggested trimming steps and trimmer positions. 3. Shave in your private areas
Implementation of Electronic Dividend Payment (“eDividend”) We are pleased to inform you of the provision of eDividend to shareholders, by Jerasia Capital Berhad (“ the Company ”). The eDividend refers to the payment of cash dividends by the Company directly into the shareholders’ bank accounts. One of the main objectives of implementing eDividend is to promote greater effici
 An extract of black, green, and mulberry teas causes malabsorptionof carbohydrate but not of triacylglycerol in healthy volunteers1–3
Litao Zhong, Julie K Furne, and Michael D Levitt
ABSTRACT
An extract of black, green, and mulberry teas causes malabsorptionof carbohydrate but not of triacylglycerol in healthy volunteers1–3
Litao Zhong, Julie K Furne, and Michael D Levitt
ABSTRACT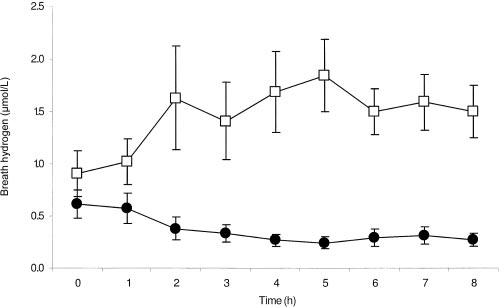
 The rice was boiled for 20 min, and then individual portions (176g containing 50 g carbohydrate) were frozen with 10 g butter.
The rice was boiled for 20 min, and then individual portions (176g containing 50 g carbohydrate) were frozen with 10 g butter.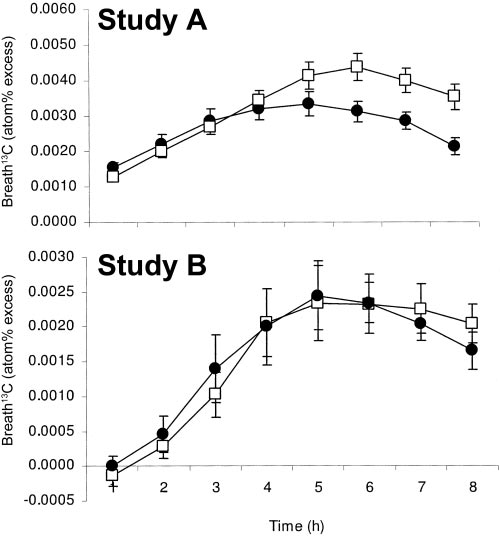
 TEA EXTRACT INDUCES MALABSORPTION OF CARBOHDYRATE
TABLE 1
TEA EXTRACT INDUCES MALABSORPTION OF CARBOHDYRATE
TABLE 1
 The carbohydrate malabsorption induced by the tea extract
indicates that carbohydrate malabsorption induced by tea ex-
was estimated by comparing the difference in breath-hydrogen
tracts also could influence blood glucose concentrations. A sim-
concentrations between the tea extract and placebo groups with
ilar observation has been reported with an extract of the root of
those observed previously (27) in healthy volunteers who in-
Salacia oblonga (44, 45). This extract reduces glucose absorp-
gested 10 g lactulose (see Equation 1). This calculation suggested
tion via inhibition of intestinal ␣-glucosidase by 2 compounds,
that Ȃ15 g of the 60 g of carbohydrate in the test meal was not
salcinol and kotanol, that differ in structure from the
absorbed. This may be a low estimate because nonabsorbed ma-
␣-glucosidase inhibitors in the tea preparation. It also should be
terial in the test meal could have been fermented less rapidly than
noted that 2 ␣-glucosidase–inhibiting drugs of bacterial origin
(acarbose and miglitol) are available for the treatment of diabe-
Elucidation of the mechanisms and specific tea extracts re-
tes. However, the use of these drugs in the United States has been
sponsible for the carbohydrate malabsorption will require addi-
limited by side effects (eg, gas and diarrhea) and by a relatively
tional studies. Mulberry leaf contains alkaloids of the
minor effect on blood glucose concentrations. The structure of
1-deoxynojirimycin type that inhibit intestinal ␣-glucosidase
␣-glucosidase inhibitors in mulberry tea differs from that of
(14). Green tea supplies epicatechin gallate and epigallocatechin
acarbose, but is similar to that of miglitol. It remains to be de-
gallate, compounds that inhibit mucosal sodium-glucose trans-
termined whether carbohydrate malabsorption induced by our
porters (17, 18). Black tea, via its theaflavin content, is an inhib-
tea extract offers any benefits over those obtained with acarbose
itor of ␣-amylase (8). The quantities of these compounds in one
or miglitol. Although a significant increase in gaseous symptoms
dose of our tea extract preparation are equivalent (depending on
was not reported after ingestion of either the tea extract or the
the compound) to that which would be contained in 5–20 cups
placebo (Table 1), studies in which tea extract is administered
(1.2– 4.8 L) of conventional tea. The extraction process reduced
with each meal should be performed before it can be claimed that
the caffeine of the tea extract to 50% of that of 1 cup (0.24 L) of
tea extract–induced carbohydrate malabsorption is associated
with fewer symptoms than has been observed with ␣-glucosi-
dase–inhibiting drugs. Indeed, it would be surprising if the de-
CO measurements did not support the concept that
gree of malabsorption observed with the tea extract (25% of total
the tea extract inhibited triacylglycerol absorption. Rather, the13
ingested carbohydrate) were not associated with some degree of
CO concentration was significantly greater when tea extract
accompanied the standard meal (Figure 2), a finding that cannot
Extracts of black, green, and mulberry teas have been con-
be explained by tea extract enhancing the absorption of lipid
sumed for many years by enormous numbers of Asians, and
because [13C]triolein absorption should approach 100% with the
these products are considered safe. Green and black tea ex-
placebo. One possible explanation is that the extract-induced
tracts also are widely used in the Western world. Although tea
carbohydrate malabsorption resulted in more rapid oxidization
extracts have been shown to interact with the metabolism of
of newly absorbed, labeled lipid because of the lesser availability
other drugs (46, 47), serious complications possibly attribut-
of glucose for energy utilization. It is also possible that the tea
able to ingestion of these extracts are rare (48). Thus, although
extract caused more rapid oxidation of absorbed [13C]oleic acid,
the potential for unintended serious side effects is seemingly
independent of differences in carbohydrate absorption (4). To
low, rare unexpected side effects of the extract can be confi-
differentiate between these 2 possibilities, 10 subjects ingested a
dently excluded only after the product has been consumed in
lipid-containing (30 g olive oil containing [13C]triolein),
an environment where medical surveillance is adequate to
carbohydrate-free meal plus the tea extract or placebo. No sig-
nificant differences in 13CO excretion were observed, which
suggested that the higher 13CO noted with the carbohydrate-
JKF helped design the protocol, recruited the subjects, and analyzed the
containing meal reflected the influence of the extract-induced
data. MDL contributed to the design of the protocol, analyzed the data, and
carbohydrate malabsorption on lipid metabolism.
The carbohydrate malabsorption induced by the tea extract
indicates that carbohydrate malabsorption induced by tea ex-
was estimated by comparing the difference in breath-hydrogen
tracts also could influence blood glucose concentrations. A sim-
concentrations between the tea extract and placebo groups with
ilar observation has been reported with an extract of the root of
those observed previously (27) in healthy volunteers who in-
Salacia oblonga (44, 45). This extract reduces glucose absorp-
gested 10 g lactulose (see Equation 1). This calculation suggested
tion via inhibition of intestinal ␣-glucosidase by 2 compounds,
that Ȃ15 g of the 60 g of carbohydrate in the test meal was not
salcinol and kotanol, that differ in structure from the
absorbed. This may be a low estimate because nonabsorbed ma-
␣-glucosidase inhibitors in the tea preparation. It also should be
terial in the test meal could have been fermented less rapidly than
noted that 2 ␣-glucosidase–inhibiting drugs of bacterial origin
(acarbose and miglitol) are available for the treatment of diabe-
Elucidation of the mechanisms and specific tea extracts re-
tes. However, the use of these drugs in the United States has been
sponsible for the carbohydrate malabsorption will require addi-
limited by side effects (eg, gas and diarrhea) and by a relatively
tional studies. Mulberry leaf contains alkaloids of the
minor effect on blood glucose concentrations. The structure of
1-deoxynojirimycin type that inhibit intestinal ␣-glucosidase
␣-glucosidase inhibitors in mulberry tea differs from that of
(14). Green tea supplies epicatechin gallate and epigallocatechin
acarbose, but is similar to that of miglitol. It remains to be de-
gallate, compounds that inhibit mucosal sodium-glucose trans-
termined whether carbohydrate malabsorption induced by our
porters (17, 18). Black tea, via its theaflavin content, is an inhib-
tea extract offers any benefits over those obtained with acarbose
itor of ␣-amylase (8). The quantities of these compounds in one
or miglitol. Although a significant increase in gaseous symptoms
dose of our tea extract preparation are equivalent (depending on
was not reported after ingestion of either the tea extract or the
the compound) to that which would be contained in 5–20 cups
placebo (Table 1), studies in which tea extract is administered
(1.2– 4.8 L) of conventional tea. The extraction process reduced
with each meal should be performed before it can be claimed that
the caffeine of the tea extract to 50% of that of 1 cup (0.24 L) of
tea extract–induced carbohydrate malabsorption is associated
with fewer symptoms than has been observed with ␣-glucosi-
dase–inhibiting drugs. Indeed, it would be surprising if the de-
CO measurements did not support the concept that
gree of malabsorption observed with the tea extract (25% of total
the tea extract inhibited triacylglycerol absorption. Rather, the13
ingested carbohydrate) were not associated with some degree of
CO concentration was significantly greater when tea extract
accompanied the standard meal (Figure 2), a finding that cannot
Extracts of black, green, and mulberry teas have been con-
be explained by tea extract enhancing the absorption of lipid
sumed for many years by enormous numbers of Asians, and
because [13C]triolein absorption should approach 100% with the
these products are considered safe. Green and black tea ex-
placebo. One possible explanation is that the extract-induced
tracts also are widely used in the Western world. Although tea
carbohydrate malabsorption resulted in more rapid oxidization
extracts have been shown to interact with the metabolism of
of newly absorbed, labeled lipid because of the lesser availability
other drugs (46, 47), serious complications possibly attribut-
of glucose for energy utilization. It is also possible that the tea
able to ingestion of these extracts are rare (48). Thus, although
extract caused more rapid oxidation of absorbed [13C]oleic acid,
the potential for unintended serious side effects is seemingly
independent of differences in carbohydrate absorption (4). To
low, rare unexpected side effects of the extract can be confi-
differentiate between these 2 possibilities, 10 subjects ingested a
dently excluded only after the product has been consumed in
lipid-containing (30 g olive oil containing [13C]triolein),
an environment where medical surveillance is adequate to
carbohydrate-free meal plus the tea extract or placebo. No sig-
nificant differences in 13CO excretion were observed, which
suggested that the higher 13CO noted with the carbohydrate-
JKF helped design the protocol, recruited the subjects, and analyzed the
containing meal reflected the influence of the extract-induced
data. MDL contributed to the design of the protocol, analyzed the data, and
carbohydrate malabsorption on lipid metabolism. TEA EXTRACT INDUCES MALABSORPTION OF CARBOHDYRATE
epigallocatechin-3-gallate and caffeine on 24 h energy expenditure and
28. Levitt MD. Production and excretion of hydrogen gas in man. N Engl
fat oxidation in men. Br J Nutr 2005;94:432– 6.
TEA EXTRACT INDUCES MALABSORPTION OF CARBOHDYRATE
epigallocatechin-3-gallate and caffeine on 24 h energy expenditure and
28. Levitt MD. Production and excretion of hydrogen gas in man. N Engl
fat oxidation in men. Br J Nutr 2005;94:432– 6.