THEODORE BENDEREV, M.D.
CERTIFIED BY THE AMERICAN BOARD OF UROLOGY
Thank you for choosing to schedule your appointment with Dr. Theodore Benderev for your vasectomy. Enclosed please find the information packet necessary to complete your chart. In order to serve you in a timely manner, we ask that you complete the information PRIOR to your appointment and bring this information back with you at the time of your appointment. Please do not mail these forms back to our office. If your paperwork is incomplete or forgotten, you may arrive 30 minutes early to fill out paperwork or we will likely have to reschedule your appointment. Please bring with you your insurance card and driver’s license. Deductibles and co-payments are due and will be collected at the time of your visit. You will be responsible for payment at the time of service if you arrive without your insurance card. Your insurance is a contract between you and your carrier. Our staff will assist you to the best of their ability in dealing with your insurance company, but it is your responsibility to know and understand your insurance policy and coverage of your plan before you arrive for your visit. If you are choosing to use your Point of Service or Out of Network Options, we recommend that you contact your insurance carrier prior to coming to our office and notify them that you are using this option for our doctors. We are located at 26732 Crown Valley Parkway (in the Mission Medical Tower), Suite #327, Mission Viejo (Our office can be reached by turning at Los Altos off of Crown Valley Parkway) and at 15775 Laguna Canyon Road, Suite 200, Irvine, CA 92618. We do not validate paid parking. Please feel free to call us at (949) 364-4400 if you have any questions. Please remember to wear long pants and wear an athletic supporter (jock strap) or tight briefs when you arrive for your procedure. Make sure that you have a light meal on the morning of the procedure.
Thank you for choosing us for your vasectomy and we look forward to serving you.
Copyright 2000-2012 Theodore Benderev, M.D. version 7.5
THEODORE V. BENDEREV, M.D. PATIENT INFORMATION SHEET - PLEASE COMPLETE IN ITS ENTIRETY LEGAL NAME - FIRST:________________________________ LAST:_________________________________________ MI_________ STREET:__________________________________________________________________________________________ SEX: F M CITY:________________________________ STATE:__________ ZIP:____________ HOME PHONE: ( )_____________________ CELL: ( ) ____________________ SOCIAL SECURITY:_______________________DATE OF BIRTH:_______________________ PREFERRED LANGUAGE: ____________________ RACE:_______________________ ETHNICITY:_______________________ EMPLOYER: ____________________________________________ JOB TITLE: ___________________________________________ EMPLOYER ADDRESS: ____________________________________________________________________________________________ WORK PHONE : ( ) ___________________________ □MARRIED □SINGLE □DIVORCED □WIDOWED YOUR PRIMARY CARE PHYSICIAN: _______________________________________ PHONE : ( )________________________ REFERRED BY (CHECK ONE): NEWSPAPER ____ WEBSITE _____ DOCTOR ____ OTHER ____________________________ REFERRING PHYSICIAN NAME: __________________________________________ PHONE: ( )__________________________ ADDRESS, CITY, STATE, ZIP: ______________________________________________________________________________________ REQUIRED TO FILL PRESCRIPTIONS PHARMACY NAME: _____________________________________________ PHONE: ( )__________________________________ ADDRESS, CITY:_________________________________________________________ FAX: ( ) ____________________________
PLEASE BRING YOUR INSURANCE CARD AND DRIVER’S LICENSE TO YOUR APPOINTMENT. IF YOU DO NOT HAVE PROOF OF INSURANCE - PAYMENT IS REQUIRED AT THE TIME SERVICE IS RENDERED. WE CAN MAKE NO EXCEPTIONS. RESPONSIBLE INSURED PARTY: (IF OTHER THAN PATIENT) FIRST NAME: _____________________________________ LAST:______________________________________ MI:_______________ RELATIONSHIP TO PATIENT: ________________________________ DRIVERS LICENSE #: ____________________________ DATE OF BIRTH: __________________________ EMPLOYER: _________________________________________________________
EMERGENCY CONTACT
NAME: __________________________________________________ PHONE : ( )________________________________________ RELATIONSHIP TO PATIENT:______________________________________________________________________________________ ASSIGNMENT & RELEASE: I HEREBY AUTHORIZE THE INCONTINENCE & PELVIC SUPPORT INSTITUTE (IPSI) TO FURNISH INFORMATION TO INSURANCE CARRIERS CONCERNING MY ILLNESS AND TREATMENTS AND IRREVOCABLY ASSIGN TO THE DOCTOR ALL PAYMENTS FOR MEDICAL SERVICES RENDERED TO ME OR MY DEPENDENTS. I HEREBY AUTHORIZE IPSI TO ACCESS, COMMUNICATE AND MAINTAIN MY MEDICATION HISTORY ELECTRONICALLY THROUGH ESCRIBE AND/OR OTHER ELECTRONIC PRESCRIPTION SERVICES IN CONNECTION WITH MY MEDICAL TREATMENT AND IN COMPLIANCE WITH HIPAA REGULATIONS. I HAVE READ AND FULLY UNDERSTAND THE FINANCIAL POLICIES. I UNDERSTAND THAT I AM RESPONSIBLE FOR ANY AMOUNT NOT COVERED BY INSURANCE. FOR ANY BALANCES OVER 45 BUSINESS DAYS OUTSTANDING, I UNDERSTAND THERE MAY BE A $5.00 MONTHLY FEE FOR BILLING SERVICE, PLUS INTEREST. A PHOTOCOPY OR SCANNED COPY OF THIS ASSIGNMENT AND RELEASE IS AS VALID AND EFFECTIVE AS THE ORIGINAL. SIGNED: _____________________________________________ DATE: _____________________
Copyright 2000-2012 Theodore Benderev, M.D. Version 7.5
A MESSAGE TO OUR PATIENTS ABOUT ARBITRATION
You will be asked to sign an arbitration agreement when you come to our office. By signing this agreement, we are agreeing that any dispute arising out of the medical services you receive is to be resolved in binding arbitration rather than a suit in court. Lawsuits are something that no one anticipates and everyone hopes to avoid. We believe the method of resolving disputes by arbitration is one of the fairest systems for both patients and physicians. Arbitration agreements between health care providers and their patients have long been recognized and approved by California courts. By signing this agreement you are changing the place where your claim will be presented. You still can call witnesses and present evidence. Each party selects an arbitrator (party arbitrators), who then select a third, neutral arbitrator. These three arbitrators hear the case. This agreement generally helps to limit the legal costs for both patients and physicians. This is because the time it takes to conduct an arbitration hearing is far less than a jury trial. Further, both parties are spared some of the rigors of trial and the publicity, which may accompany judicial proceedings. Our goal, of course, is to provide medical care in such a way as to avoid any such dispute. We know that most problems begin with communication. Therefore, if you have any questions about your care, please ask.
Copyright 2000-2012 Theodore Benderev, M.D. Version 7.5
THEODORE V. BENDEREV, M.D. FINANCIAL POLICIES
We welcome you to our office. We are able to concentrate on the practice of medicine and provide quality care by having our financial policies understood by our patients and by avoiding confusion or misunderstandings. Filing insurance claims is a courtesy extended to our patients and is not a guarantee of payment. We will bill insurance claims with a maximum of two insurance carriers per patient. It is important to emphasize that your insurance is a contract between you and the insurance carrier. Insurance plans and contracts change constantly. It is your responsibility to contact your insurance company and verify your benefits and verify that your doctor is a contracted provider in your network PRIOR to your visit. You will be financially responsible for the services rendered if we have not been paid by your insurance carrier within 45 business days. _________ (patient’s initials) Drs. Benderev is a participating physician with Medicare and accepts assignment for all covered Medicare services. Medicare pays 80% of approved charges and the patient is responsible for the other 20%, after the annual deductible is met. Our office staff will bill secondary insurance if the responsible party has given permission to the insurance company to have the payment sent to us. Dr. Benderev is not a participating physician with Medi-Cal and therefore, cannot accept Medi-Cal insurance (including retro-active Medi-Cal coverage). For patients without insurance plans or for patients that are unable to provide an insurance card verifying current coverage, we require payment at the time services are rendered. If you do not have insurance or your insurance company does not pay for services rendered it is the patient’s responsibility for payment in full. This also applies to patients requesting services that have insurance plans with which we are not contracted, (e.g., out-of-network coverage). ______ (patient’s initials)
All services rendered by Dr. Benderev that is not a covered benefit of your insurance policy is your responsibility to pay. Any patient that is seen or treated without proper authorization from their insurance carrier is responsible for the full charge of the services rendered if no payment is authorized retrospectively. All monies owed by the patient (e.g. co-payments, deductibles, required “out-of-pocket” amounts, non- covered services and co-insurance amounts) are due at the time services are rendered. _________ (patient’s initials) If your account is placed with a collection agency, due to non-payment, you will be responsible for any additional charges this may incur, including a monthly interest and penalty fee, collection agency fees, attorney fees, court fees, and any other fees associated in collecting the balance due. _________ (patient’s initials) While we understand there may be times when our patients need to cancel their appointments, we have found it necessary to implement a “Cancellation and No-Show Policy”. Any patient who fails to arrive for a scheduled appointment without canceling the appointment at least 24 hours prior to the scheduled time is considered a “no-show.” A no-show patient scheduled for an office visit may be charged $40.00. A no- show patient scheduled for a procedure or diagnostic test may be charged $100.00. No-show charges are not billable to your insurance company and are your responsibility to pay. _________ (patient’s initials) We are willing to work with any patient requesting a financial payment plan. There will be a $45 charge for each check that is returned for insufficient funds. We hope you find this information helpful. Please feel free to ask our office staff if you require any further assistance. Patient Signature:_____________________________________ Date:_________________________
Copyright 2000-2012 Theodore Benderev, M.D. Version 7.5
PRECAUTIONS FOR SURGERY
All patients anticipating surgical procedures must stop taking aspirin and aspirin products as well as ibuprophen for 10-14 days prior to procedure. These drugs and other nonsteroidal anti- inflammatory drugs are anticoagulants (blood thinners) which can cause bleeding problems during and following the procedure. THE FOLLOWING COMPOUNDS ARE TO BE AVOIDED: FOR 10 TO 14 DAYS PRIOR TO SURGERY.
(Contact your general physician if there is any question whether you need the medicine.)
ALSO AVOID “HERBAL” COMPOUNDS PRIOR TO SURGERY.
A number of herbal remedies have side effects that could complicate surgical procedures by inhibiting blood clotting, affecting blood pressure, or interfering with anesthetics. Ginkgo biloba, feverfew, garlic, ginger, and ginseng have all been shown to interfere with the function of platelets - necessary for clotting. The use of herbal preparations in the United States has risen dramatically over the past decade. Although we do not have the exact rate of complications form herbs, the potential for them to cause a problem is real.
Copyright 2000-2012 Theodore Benderev, M.D. Version 7.5
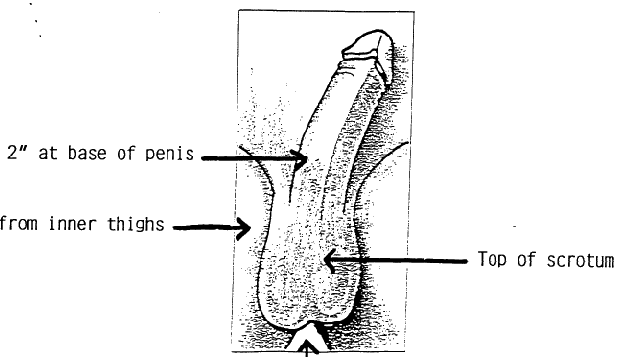
SHAVING / CLIPPING INSTRUCTIONS FOR THE DAY OF VASECTOMY On the day of the procedure you should (shave or) preferably clip the hair at the bottom 2 inches of the penis and the top/front of the scrotum. PLEASE CLIP OR SHAVE ON THE DAY OF THE PROCEDURE, NOT THE NIGHT BEFORE. ALSO, PLEASE REMEMBER TO WEAR AN ATHLETIC SUPPORTER OR TIGHT BRIEFS WHEN YOU COME FOR YOUR PROCEDURE.
Copyright 2000-2012 Theodore Benderev, M.D. Version 7.5
Theodore Val Benderev, M.D. PATIENT VASECTOMY QUESTIONNAIRE
Patient Name: ____________________________________ Date: _______________________ Referred by: ________________________________ Age: _______ years old Describe the health care that you are seeking today: (Chief Complaint) ____________________________________________________________________________
VASECTOMY HISTORY
Is there anyone in your family who has had prostate cancer?
Have you had an infection in the testicle area? Yes No
If so, which relative was is he? ______________
Have you had any conditions affecting the urine, kidneys,
If yes, what medication were you treated with and for how
________________________________________________
________________________________________________
________________________________________________
How long ago did you first consider a vasectomy?
Have you ever been injured in the scrotal area? Yes No
___ weeks ago ___ month(s) ago ___ year(s) ago
If so, describe__________________________________
Please indicate if you have reviewed information on either
Have you ever had an inguinal hernia repair? Yes No
What, if any, additional questions or concerns do you have?
Does your wife / partner wish for you to
________________________________________________
Past Illnesses – please circle all that apply and list others:
Past Surgeries – list any operations you have had and the year of each procedure
_____________________________________________________________________________________________________________________________ _____________________________________________________________________________________________ Medications – list all prescription and non-prescription medications you use with theirdoses:
(include aspirin, hormones, birth control pills, laxatives, vitamins, calcium and others)
_______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Copyright 2000-2012 Theodore Benderev, M.D. Version 7.5
Patient Name: __________________________________________________ Date: ______________________
ALLERGIES (include medication, iodine, seafood, latex & others) REACTION
____________________________________________________________________________________________ _____________________________________________________________________________________________ Your Family’s Medical History – list illnesses of your blood relatives (include heart disease, diabetes, high blood pressure, bleeding problems) relations Deceased relations Illness/Cause of death
__________________________________________ ______________________________________________ __________________________________________ ______________________________________________ Social History – please circle or fill in the blank.
Marital status: Single Married Happily Married Unhappily Separated
How many children do you have? From this marriage ______ From Prior Marriage: ______ Age Range _____________
Your occupation: __________________________ Are you retired? Yes No
Tobacco use: Never Smoker Former Smoker Current some day smoker Current Every Day Smoker
Never drinks Drinks rarely ___ drinks per week
Review of Systems Please circle all symptoms that you currently have:
Copyright 2000-2012 Theodore Benderev, M.D. Version 7.5
Theodore V. Benderev, M.D. CONFIDENTIAL COMMUNICATION REQUEST
I, ________________________________ (print name) hereby request the use of the following confidential channels for the communication of information related to my personal health, treatment or payment for treatment. This request supercedes any prior request I may have made for confidential channel communications. Please answer the following two questions by selecting YES or NO. If you choose to have us leave messages for you, please note those numbers below. PHONE MESSAGES AND DETAILED INFORMATION I authorize Drs. Benderev and his agents to leave a voice message regarding non-clinical and clinical information at this number: __YES or __NO Phone #: _________________________.
An example of clinical information would be lab or x-ray results, etc. An example
of non-clinical information would be appointment reminders. -----------------------------------------------------
I authorize Drs. Benderev and his agents to leave a non-clinical message only at this number: __YES or __NO Phone #: _________________________. Signed: __________________________ Date:
Copyright 2000-2012 Theodore Benderev, M.D. Version 7.5
INCONTINENCE & PELVIC SUPPORT INSTITUTE NOTICE OF PRIVACY PRACTICES ACKNOWLEDGEMENT OF RECEIPT
By signing this form, you acknowledge receipt of the Notice of PrivacyPractices of the Incontinence & Pelvic Support Institute. Our Notice of Privacy Practices provides information about how we may use and disclose your protected health information. We encourage you to read it in full. Our Notice of Privacy Practices is subject to change. If we change our notice, you may obtain a copy of the revised notice by contacting our Privacy Officer at 949/364-4400. I acknowledge receipt of the Notice of Privacy Practices of the Incontinence & Pelvic Support Institute. Signature: ______________________________________ FOR OFFICE USE ONLY
INABILITY TO OBTAIN ACKNOWLEDGEMENT To be completed only if no signature is obtained. If it is not possible to obtain the individual’s acknowledgement, describe the good faith efforts made to obtain the individual’s acknowledgement, and the reason why the acknowledgement was not obtained: Signature of provider representative: ________________________________
Communication barriers prohibited obtaining the acknowledgement
An emergency situation prevented us from obtaining acknowledgement
Other (please specify): ___________________________________________________________
______________________________________________________________________________________ ______________________________________________________________________________________
Copyright 2000-2012 Theodore Benderev, M.D. Version 7.5
Bellevue University Tobacco Free FAQ’s Q: What does a tobacco-free campus mean? What areas of campus does this entail? A: The use of tobacco is prohibited within the university campus. This includes all buildings, parking structures, campus walkways, and university-owned vehicles. This policy applies to all students, faculty, staff, vendors and other visitors to all university propert
Vortrag: Dr. A. Bau München, 18. 10. 2005 Von der Verhaltensauffälligkeit zur Krankheit. Medizinalisierung und Psychiatrisierung der Kinder. Am Beispiel des Aufmerksamkeits-Defizit-Hyperaktivitäts-Syndroms (ADH-Syndrom). 1). Einführung, Geschichtliches, wie kommt es zur „Diagnose“ „ADH“ Seit einigen Jahren beobachten wir Ärzte, Eltern, Kindergärtnerinnen und Lehrer be
 SHAVING / CLIPPING INSTRUCTIONS
SHAVING / CLIPPING INSTRUCTIONS