Some of the important complications include infections, blood clots, inadvertent injury to blood vessels or nerves, problems regaining flexion or extension of the knee and difficulties with wound healing. Deep infec-tion may require removal of the implant, prolonged antibiotics and later surgery to insert a new implant. Major clots are rare but can be fatal. All surgery and anaesthesia carries risks and it is not entered into lightly. Dr Coolican and his surgical team work very hard to prevent complications and it is important that you cooperate with all medical and paramedical staff to achieve an optimum result. If you have any questions
concerning complications, please feel free to speak
with Dr Coolican. If you develop unexplained calf pain, chest pain, fever or wound redness, please notify Dr Coolican or the hospital staff.
Precautions after Surgery:
You should avoid impact and jarring activities. You are not able to run with your prosthesis. Dr Coolican will
be happy to provide you with a list of activities which
you can carry out safely after knee replacement but it is important that you have one foot on the ground at all
Repl acem ent
times. Accordingly, you should not run or jump.
In the first year or two after surgery, you should tell your dentist if you have any dental work, so that antibi-otics can be provided to prevent secondary infection in the knee. This is the case for any open surgery and you should ensure prompt antibiotic treatment of any skin infection or urinary tract infection.
Dr Coolican’s fees are above the Medicare schedule.
This will produce a gap payment for your surgery and Dr Coolican’s secretary will inform you of the gap.
If you have any questions concerning your forthcom-
ing knee replacement, including risks, complications or
likely outcome, please do not hesitate to contact Dr
Introduction Rehabilitation
care are carried out. You will also be given a PCA button
Total knee replacement (TKR) is major surgery and a
which delivers a small volume of narcotic intravenously.
Most patients require a more prolonged stay in hospital
decision to proceed with the operation is made only
for intensive physiotherapy. This is usually arranged if
after a thorough consideration of the symptoms you are
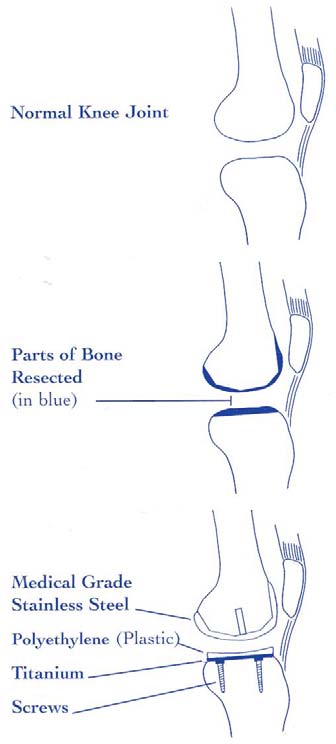
Surgery is carried out through an incision over the front of the
necessary in a rehabilitation hospital. We utilize a num-
suffering and the likely risks and benefits of surgery.
knee and takes approximately one to two hours, depending
ber of different hospitals, depending on your needs and
on what is required. Small parts of the ends of the bones
Prior to booking surgery, Dr Coolican will question you
the area where you live. Most patients require some
(femur and tibia) are removed and replaced with prostheses
on your general health. If there is a history of medical
form of walking aid – crutches, frame or a stick for the
matched for size and side. The patella may be resurfaced,
problems, such as troubles with your heart, lungs, blood
first three months or thereabouts although people vary
depending on the findings at surgery and your preoperative
pressure, kidneys, circulation or other health issues,
with this. It is entirely up to the patient’s confidence al-
clinical features. The prostheses are fixed to your bone either
you may be referred to an appropriate specialist for an
though a stick outside the home is a good idea for the
by bone cement or a press fit where the bone grows into po-
opinion on whether you are fit for the surgery and
first three months as it alerts others that you are not fully
rous surface on the undersurface of the prosthesis. There is
whether any special precautions are required. If you
mobile and able bodied. Injections of low molecular
not yet a clear consensus that either form of fixation gives
are considered unfit or the specialist considers the risk
weight heparin (usually Clexane) continue until transfer to
better long term results. A low pressure suction drain is util-
of surgery to be great, it may still be possible to proceed
rehabilitation and you should continue with the white
ized to remove shed blood from the joint and the shed blood
with surgery but only after you and your relatives are
(TED) stockings until the 6 week postoperative check. At
can be stored, filtered and retransfused if suitable.
aware of and are prepared to accept the risks.
this appointment, further radiographs are taken of your
Most patients recovering from total knee replacement find the
Please stop any aspirin containing medication that you
knee to be quite uncomfortable in the first two weeks. A vari-
have been taking 10 days prior to surgery. Non-
Most patients can safely drive at 6 weeks and gradually
ety of measures are used to control pain, including continu-
steroidal anti-inflammatories should also be stopped 10
increasing walking distances occur around this time.
ous epidural infusion (similar to that used in childbirth), pa-
days prior to surgery. These drugs interfere with the
Bowls and golf can be resumed whenever you feel confi-
tient controlled analgesia, nerve block injections, ice and oral
clotting mechanism. You should continue with all your
dent, usually somewhere between 3 and 6 months. Run-
medications. It usually takes between 2 and 12 months be-
other medications and bring them to hospital, so that
ning is not permitted at any time after the operation as
fore the patient agrees that the replaced knee feels better
the staff can arrange ongoing prescription at the appro-
wear of the prosthesis occurs very quickly. You may be
than before surgery but this is variable. Some patients will
priate dose. You must also bring your x-rays and other
able to drive an automatic car sooner than 6 weeks post-
have very little pain after surgery and wonder what all the
imaging scans. If you are taking aspirin or Plavix for a
operatively if your left knee has been replaced but stud-
fuss is about whilst others, are troubled by quite severe night
special reason that makes it dangerous to stop, it may
ies are suggestive that it takes most patients around 6
pain for two or three months after surgery.
be necessary to continue with this medication up to
weeks before they can confidently operate the pedals
surgery but this should be discussed with Dr Coolican.
The day after surgery, the nursing staff will remove the drain
with sufficient power and speed to drive safely.
If you are taking Warfarin, specific arrangement, de-
and dressings and apply TED stockings. Although this is a
pending on the requirements for Warfarin will be made.
relative rest day, it is important to wiggle your ankles up and
Results and Complications:
It is usual to stop the Warfarin 5 days or thereabouts
down a few times, every 20 minutes or so whilst you are
before surgery and continue without anticoagulation or
awake. This helps the calf muscle pump and prevents clots.
Overall, 95% of patients are happy with the knee replace-
possibly continue with some form of anticoagulation
Usually, the nursing staff and physiotherapist will sit you over
ment. Approximately 90 – 95% are relieved of the major-
injection in the period up to the surgery.
the side of the bed on the first postoperative day and you may
ity of their pain. The deformity (crookedness) of the leg is
corrected and mobility is improved. Range of motion
Hospital
averages around 115° but patients with poor motion prior
On the second postoperative day, rehabilitation begins in
to surgery seldom achieve a large improvement.
earnest. This is supervised by the physiotherapist and in-
You are usually admitted to hospital the day before sur-
volves a series of exercises to achieve two goals. These are
Should the prosthesis wear out, revision knee replace-
gery or occasionally on the same day. Prior to this, you
to get the knee bending and to improve independent mobility.
ment is possible but is more complex surgery than the
will attend a preadmission clinic which will involve blood
A continuous passive motion (CPM) machine may be used in
first replacement with results not being in general as sat-
tests, an ECG and chest X-ray. You will also meet the
order to obtain knee bend. These are electric operated ma-
isfactory as first time surgery. The risks of revision sur-
chines placed on the bed with the machine moving the knee
On the day of surgery, your leg is washed, shaved if
up and down. Controls determine the degree of motion and
The prosthesis is a mechanical device with a bearing
necessary and painted with antiseptic solution. The leg
the patient holds a stop button. CPM machines are not al-
surface which wears out over time. Mostly the implant
is then wrapped in a sterile towel. You will meet the
ways utilized and depends on progress with range of motion.
will out survive the patient. Failure occurs due to wearing
anaesthetist prior to surgery who will discuss the anaes-
Discharge from hospital occurs when the knee is bending
out of the plastic component or the implant works loose in
thetic with you. This usually takes the form of a general
adequately and you are mobile, either on crutches or a frame
the bone. Too high an activity level and soft bone (e.g.
anaesthetic and something else to control pain after the
and can safely get about. The average length of hospital stay
due to rheumatoid arthritis) are factors in an implant re-
surgery. This may be an epidural or spinal injection,
is a week or a shade under and has reduced over time. You
quiring revision. Avoiding excessive weight gain is also
nerve block, nerve catheter or local anaesthetic around
may be required to stay in hospital longer if complications or
the knee. Varieties of these forms of postoperative pain
PRESS RELEASE Addex Therapeutics Awarded $1 MM Grant from The Michael J. Fox Foundation for Parkinson’s Research Grant to be used to help fund further human clinical testing of dipraglurant for the treatment of Parkinson’s disease levodopa-induced dyskinesia New York, NY and Geneva, Switzerland, 19 March 2013 – Addex Therapeutics (SIX: ADXN), a leading compan
Glossary of terms relating to mental hospitals, Western Australia Antipsychotic A class of drugs developed in the early 1950s which seemed to control the more distressing symptoms of psychotic illness. The first modern antipsychotic was chlorpromazine . Bromo-chloral, pot. brom chloral A combination of chloral hydrate and potassium bromide, used as a sedative in general, maternity
 Some of the important complications include infections, blood clots, inadvertent injury to blood vessels or nerves, problems regaining flexion or extension of the knee and difficulties with wound healing. Deep infec-tion may require removal of the implant, prolonged antibiotics and later surgery to insert a new implant. Major clots are rare but can be fatal. All surgery and anaesthesia carries risks and it is not entered into lightly. Dr Coolican and his surgical team work very hard to prevent complications and it is important that you cooperate with all medical and paramedical staff to achieve an optimum result. If you have any questions
concerning complications, please feel free to speak
with Dr Coolican. If you develop unexplained calf pain, chest pain, fever or wound redness, please notify Dr Coolican or the hospital staff.
Precautions after Surgery:
Some of the important complications include infections, blood clots, inadvertent injury to blood vessels or nerves, problems regaining flexion or extension of the knee and difficulties with wound healing. Deep infec-tion may require removal of the implant, prolonged antibiotics and later surgery to insert a new implant. Major clots are rare but can be fatal. All surgery and anaesthesia carries risks and it is not entered into lightly. Dr Coolican and his surgical team work very hard to prevent complications and it is important that you cooperate with all medical and paramedical staff to achieve an optimum result. If you have any questions
concerning complications, please feel free to speak
with Dr Coolican. If you develop unexplained calf pain, chest pain, fever or wound redness, please notify Dr Coolican or the hospital staff.
Precautions after Surgery: