Microsoft word - sec 09.9.form 209 forms v1.3 _2004 03-26_.doc
Section 9: Forms Completion and Data Submission
Form 209 – Medications
Section 9: Forms Completion and Data Submission
Form 209 – Medications (continued)
Section 9: Forms Completion and Data Submission
Form 209 – Medications Submission: Completed by: When to complete
At each Six Month and Annual Visit or Contact
and submit: Contact Number:
016, 020, 026, 030, 036, 040, 046, 050, 056, 060, 066, 070, 076, 080 (the following may be applicable depending on the time-point of the study when the participant was randomized) 086, 090, 096, 100, 106, 110, 116, 120, 126, and 130.
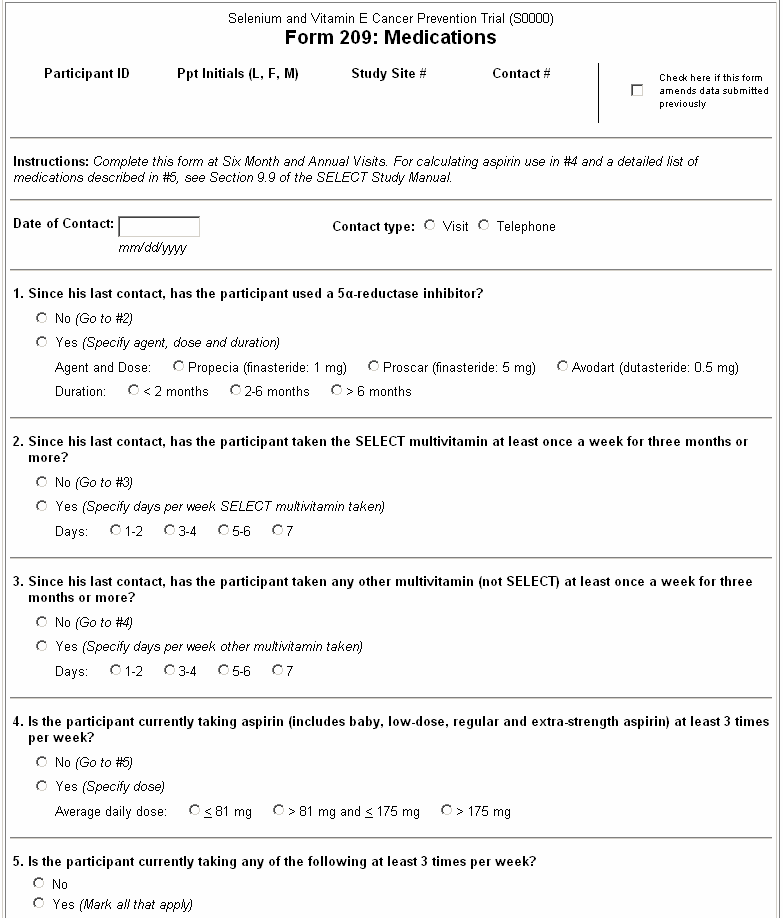
Form Instructions: 1. Since his last contact, has the participant used a 5α-reductase inhibitor?
If response is Yes, select one response each to indicate the specific Agent and Dose and Duration. 2. Since his last contact, has the participant taken the SELECT multivitamin at least once a week for three months or more? If response is Yes, then mark the number of days the participant took the SELECT multivitamin during the period he was taking it. The participant should indicate whether he took the SELECT multivitamin at least once a week for three months or more in the past six months. The three months do not need to be contiguous. Example: A participant took multivitamins daily for one month, stopped taking them for three months, then took multivitamins again daily for two months. Check Yes in question #2, then check “7” to specify the number of days per week he took the SELECT multivitamin.
3. Since his last contact, has the participant taken any other multivitamin (not SELECT) at least once a week for three months or more? If response is Yes, then mark the number of days the participant took the other multivitamin during the period he was taking it.
The participant should indicate whether he took the other multivitamin at least once a week for three months or more in the past six months. The three months do not need to be contiguous. Multivitamins are mixtures containing 10 or more different vitamins or minerals.
4. Is the participant currently taking aspirin (includes baby, low-dose, regular and extra- strength aspirin) at least 3 times per week? Select Yes if participant is taking aspirin or medications containing aspirin at least 3 times a week. Refer to the Aspirin Consumption Table in the form instructtion #8, to estimate daily dose.
Section 9: Forms Completion and Data Submission
Specify participant daily dose as follows:
Average dose ≤ 81 mg per day Average dose > 81 mg and ≤ 175 mg per day Average dose > 175 mg per day See the form on #8, for more information on calculating average aspirin consumption and a partial listing of brand names for aspirin to assist with answering this question. 5. Is the participant currently taking any of the following at least 3 times per week?
If response is Yes, select all types of medication listed that the participant currently takes at least 3 times a week. See the following medication list for reference. If the participant is taking a medication for indications other than listed below, that medication should be recorded on Question #5. Any indications listed below are for reference only. Do not use the Comments section as a medication log. The medication log is a separate piece of source documentation that is maintained independently of the data recorded on this form. Form 209 Medication list to assist with answering Question #5: This is a partial listing of medications for each category of medication associated with Question #5. Brand names are listed in italics. Anti-inflammatory drugs in the COX–2 inhibitors class: Celecoxib (Celebrex) Rofecoxib (Vioxx) Valdecoxib (Bextra) Other non-steroidal anti-inflammatory drugs (NSAIDS): The NSAIDS category deliberately excludes aspirins such as Anacin, Ascriptin, Bayer, Bufferin, Excedrin and Ecotrin because aspirin is included in another category. Similarly, NSAIDS that are also Cox II inhibitors have been excluded from this list. If the participant currently takes any of the aspirin products listed in Question #4, do not indicate Yes in the “Other NSAIDS” category unless he also takes an NSAID listed below. Diclofenac (Voltaren, Cataflam) Diflunisal (Dolobid) Ibuprofen (Advil, Nuprin, Motrin, Pamprin, Rufen, Midol, Medipren and generic brands) Indomethacin (Indocin) Ketorolac (Toradol) Mefenamicacid (Ponstel) Nabumetone (Relafen) Naproxen (Naprosyn, Naprelan, Anaprox, Aleve) Piroxicam (Feldene) Salicylate derivatives (Trilisate) Sulindac (Clinoril)
Section 9: Forms Completion and Data Submission
Lipid-lowering agents of the Statin class: Atorvastatin (Lipitor) Fluvastatin (Lescol) Lovastatin (Mevacor) Lovastatin Extended-Release (Altocor) Niacin & Lovastatin (Advicor) Pravastatin (Pravacohol) Simvastatin (Zocor) Clopidogrel (Plavix) for blood thinning: Clopidogrel (Plavix) Gastric acid reducing agents of the Histamine 2 antagonist class: Cimetidine (Tagamet) Famotidine (Pepcid) Nizatidine (Axid) Ranitidine (Zantac)
EC safety data sheet Trade name: Bicalutamide 50 mg Film-coated tablets / Bicalutamide 150 mg Film Identification of the substance/preparation and of the company/undertaking Identification of the substance or preparation Trade name Bicalutamide 50 mg Film-coated tablets / Bicalutamide 150 mg Film coated tablets Use of the substance/preparation Company/undertaking i
Institución Educativa Escuela Normal Superior Resolución Aprobación Nro.006990 de Sept.07/92 Acreditación MEN Resolución Nro. 3684 de Dic. 09/98 INSTITUCIÓN EDUCATIVA ESCUELA NORMAL SUPERIOR MARÍA AUXILIADORA INFORME DE GESTIÓN VIGENCIA 2011 Copacabana, febrero 16 de 2012 Presentación Hna Sara Cecilia Sierra Jaramil o, con Cédula de ciudadanía Nº 42 679 309, del munici
 Section 9: Forms Completion and Data Submission
Form 209 – Medications
Section 9: Forms Completion and Data Submission
Form 209 – Medications 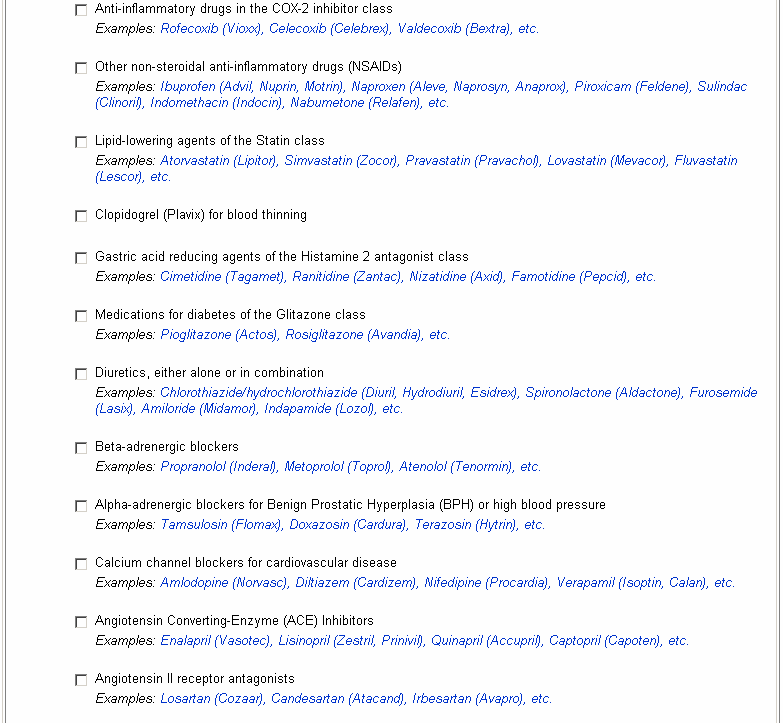

 Section 9: Forms Completion and Data Submission
Form 209 – Medications (continued)
Section 9: Forms Completion and Data Submission
Form 209 – Medications (continued)