Psychological Medicine, 2001, 31, 1331–1345.
DOI : 10.1017\S0033291701004664 Printed in the United Kingdom
The neuroendocrinology of chronic fatigue syndrome and
A. J. R. P A R K E R , S. W E S S E L Y A. J. CLEARE"
From the Department of Psychological Medicine, Guy’s, King’s and St Thomas’ School of Medicine and theInstitute of Psychiatry, LondonABSTRACT Background.
Disturbance of the HPA axis may be important in the pathophysiology of chronic
fatigue syndrome (CFS) and fibromyalgia. Symptoms may be due to : (1) low circulating cortisol ;(2) disturbance of central neurotransmitters ; or (3) disturbance of the relationship between cortisoland central neurotransmitter function. Accumulating evidence of the complex relationship betweencortisol and 5-HT function, make some form of hypothesis (3) most likely. We review themethodology and results of studies of the HPA and other neuroendocrine axes in CFS.
Medline, Embase and Psychlit were searched using the Cochrane Collaboration strategy.
A search was also performed on the King’s College CFS database, which includes over 3000relevant references, and a citation analysis was run on the key paper (Demitrack et al. 1991). Results.
One-third of the studies reporting baseline cortisol found it to be significantly low, usually
in one-third of patients. Methodological differences may account for some of the varying results. More consistent is the finding of reduced HPA function, and enhanced 5-HT function onneuroendocrine challenge tests. The opioid system, and arginine vasopressin (AVP) may also beabnormal, though the growth hormone (GH) axis appears to be intact, in CFS. Conclusions.
The significance of these changes, remains unclear. We have little understanding of
how neuroendocrine changes relate to the experience of symptoms, and it is unclear whether thesechanges are primary, or secondary to behavioural changes in sleep or exercise. Longitudinal studiesof populations at risk for CFS will help to resolve these issues.
heated debate between sufferers, doctors and the
INTRODUCTION
media (Wessely et al. 1998). While psychiatrists
Chronic fatigue syndrome (CFS) is defined as
have been keen to emphasize its close relation to
medically unexplained, disabling fatigue of 6
psychiatric disorders – depression is present in
months or more duration, often accompanied
about 50 % (David, 199l) – sufferers often main-
by several of a long list of physical complaints
tain that their fatigue has a solely physical cause,
(Fukuda et al. 1994 ; Sharpe et al. 1991). It is
perhaps viral. Epstein–Barr virus has been
relatively common, with a prevalence of around
shown to be a risk factor for CFS (White et al.
0n5% in primary care (Wessely et al. 1998) and
1998), though epidemiological studies suggest
poor spontaneous recovery at 18 months follow-
that viruses can not account for the majority of
up (Vercoulen et al. 1996). Discussion of its
cases (Horwitz et al. 1985 ; Holmes et al. 1987 ;
nature and causes has initiated occasionally
Buchwald et al. 1987). Findings from immuno-logical studies have also been non-specific and
" Address for correspondence: Dr A. J. Cleare, Section of
inconsistent (Wessely et al. 1998).
Neurobiology of Mood Disorders, Academic Department of
Psychological Medicine, GKT School of Medicine and Institute ofPsychiatry, 103, Denmark Hill, London SE5 8AF.
nature of CFS is the hypothalamic–pituitary–
adrenal axis (HPA). Interest led from observa-
tions that conditions of low circulating cortisol
are characterized by debilitating fatigue, forexample in Addison’s disease, and following
bilateral adrenalectomy (Riordain et al. 1994).
These conditions also share other symptoms
with CFS, such as arthralgias, myalgias andsleep and mood disorder (Baxter & Tyrell,
1981). It has therefore been suggested that thefatigue of CFS is mediated by low circulating
levels of cortisol. This hypothesis has gainedcredence in the last decade or so, though a
glance at history shows that it is not in fact new. From 1902 to 1925 the term hypoadrenia or ‘ a
bit of Addison’s disease ’ held sway as thediagnosis of the time for such symptoms, thoughwithout firm scientific grounding (Tattersall,1999).
Recent interest in cortisol and the HPA axis in
CFS has applied greater scrutiny to the hy-potheses. Poteliakhoff was the first to dem-
onstrate significantly lower baseline cortisol in
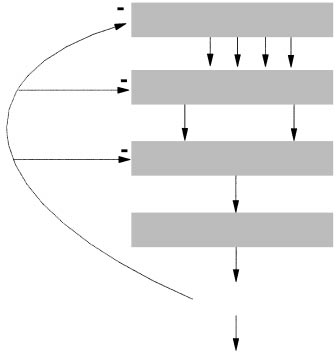
F. 1. The hypothalamic–pituitary–adrenal axis. (GR, Glucocorti-
patients with chronic fatigue, compared to
coid ; MR, mineralcorticoid ; CRH, corticotrophin releasing hor-
controls (Poteliakhoff, 1981). However, since
mone ; AVP, arginine vasopressin ; ACTH, adrenocorticotrophic
then, attempts to replicate and extend Poteli-
akhoff’s findings have been far from straight-forward. This review examines the current
interactions are complex and not yet fully
evidence for neuroendocrine disturbance in CFS,
understood, though hippocampal 5-HT" re-
highlighting the methodological problems that
ceptors are thought to be of central importance
have hampered consistency, but also led to
and are involved in controlling CRH release
greater appreciation of the complexity of the
from the hypothalamus (Lesch et al. 1990). 5-
neuroendocrine\behavioural interplay.
HT system modulation of the HPA probablyextends beyond the hippocampus, as 5-HT isalso thought to stimulate ACTH release at
OVERVIEW OF THE HPA
hypothalamic and pituitary levels. In turn,
The HPA axis is the primary endocrine stress
circulating cortisol, regulates central 5-HT sys-
axis in man. Secretion of cortisol from the
tem activity, as well as directly inhibiting the
adrenal cortex is regulated by a complex system
release of CRH and ACTH (Dinan, 1996). In
of long and short feedback loops. Corticotrophin
depression, both 5-HT system down-regulation
releasing hormone (CRH) and arginine vaso-
pressin (AVP), released by the hypothalamus act
prominent neuroendocrine hypotheses over the
synergistically to regulate the output of adreno-
last decade. Advances in the understanding of
corticotrophic hormone (ACTH) from the an-
the relationship between these two systems allow
terior pituitary. In the systemic circulation
a preliminary synthesis with implications for the
ACTH acts at the adrenal cortex stimulating the
treatment of depression (McAllister-Williams &
release of cortisol, which has a negative feedback
effect at hypothalamic and pituitary levels,decreasing the output of CRH, AVP and ACTH.
centrally via the hippocampus, partly through
Medline, Embase and Psychlit were searched
reciprocal interactions with the 5-HT (serotonin)
using the Cochrane Collaboration search strat-
system (Chaouloff, 1993). The HPA – 5-HT
egy for CFS (available from authors), linked to
a key word search for relevant neuroendocrine
ACTH, cortisol responses were significantly
lower than controls, suggesting an overall
CRH, synacthen, neuroendocrine, neuroendo-
reduced maximal secretory capacity of the
crinology, hypothalamus, pituitary, adrenal,
adrenal cortex. On stimulation with ovine CRH,
growth hormone, IGF), for the years 1966–1999.
subjects with CFS had significantly attenuated
A second search was performed on the King’s
ACTH responses, but cortisol responses were
College CFS database, which has been main-
similar to controls, demonstrating proportion-
tained (by S. W.) since 1991 with over 3000
ately higher cortisol secretion per unit of
relevant references. Finally, a citation analysis
ACTH – further evidence for hypersensitivity of
was run on the key relevant paper (Demitrack et
the adrenal cortex to ACTH. These findings led
the NIH group to suggest that the hyper-responsiveness of the adrenal cortex in subjectswith CFS was secondary to increased sensitivity
SETTING THE SCENE : THE NIH
of ACTH receptors due to chronically inad-
RESEARCH
equate levels of ACTH. Further, they hypothe-
The most comprehensive study of the HPA axis
sized that the decreased maximal cortisol re-
in CFS remains that of Demitrack and colleagues
at the National Institute of Health, USA – the
atrophy of the adrenal cortex itself, again
NIH study (Demitrack et al. 1991). They studied
consequent upon chronically inadequate levels
30 CFS patients and 72 normal controls, in a
complex design that included baseline measures
hypocortisolism reflects a defect at or above the
of cortisol, ACTH and cortisol-binding globulin
level of the hypothalamus resulting in a defi-
(CBG). They also evaluated the response of the
ciency in CRH and\or other secretagogues that
HPA axis to challenge tests, using ovine CRH
serve to activate the pituitary–adrenal axis. Their
evidence was inconsistent with either a primary
to controls, patients with CFS showed re-
adrenal insufficiency or impairment of the
ductions of approximately 40 % in evening basal
plasma cortisol and 24 h urinary free cortisol
One finding which is not consistent with the
NIH group’s interpretation, though, is the raised
creased, it was concluded that basal cortisol
evening ACTH – in contrast to the chronically
levels were low throughout the day, and not
low levels that they hypothesize. However,
only in the evening as reflected in the low basal
although three plasma samples were taken for
plasma sample. In addition, significantly higher
levels of CBG were found in CFS subjects. This
evening. This is undoubtedly inadequate for a
may relate to a decreased cortisol effect con-
hormone with a known diurnal variation, and a
sidering the evidence in rodents (Fleshner et al.
pulsatile nature of release (Pincus et al. 1999).
1995 ; Spencer et al. 1996) and in humans
The radio-immune assay employed is also likely
(Schlecte & Hamilton 1987 ; Gala & Westphal,
to be less reliable than more recently developed
l966), for a negative feedback of circulating
assays for ACTH (Kertesz et al. 1998).
glucocorticoids on CBG levels. Also significantly
raised in CFS subjects were basal levels of
major hypotheses in need of further study. First,
ACTH, suggesting that the cortisol deficiency
that in CFS, the experience of fatigue is mediated
was not secondary to under-functioning pitu-
by inadequate levels of circulating cortisol, and
a reduced ability to mount an adequate cortisol
On challenge with ACTH, cortisol responses
response to stress. This remains an appealing
were proportional to the dose of ACTH in all
hypothesis considering the clinical correlation
subjects. However, at low doses of ACTH, only
with medical conditions of low circulating
CFS subjects showed cortisol rises above pla-
cortisol. How the lack of cortisol exerts this
cebo, suggesting a hypersensitivity of the adrenal
effect warrants further study – is it centrally,
cortex to ACTH compared with controls. This
peripherally, or a combination of both? The
would be incompatible with a primary adrenal
second hypothesis is that the fatigue is centrally
insufficiency. In contrast, at higher doses of
mediated, not by low cortisol itself, but by
reduced CRH or other mediators controlling the
Salivary cortisol is arguably a better way to
HPA axis. Although central neurohormones\
measure baseline cortisol, since as well as being
neurotransmitters cannot be measured directly
non-invasive, it is thought to provide a more
in humans, indirect evidence suggests that these
accurate and valid measure of biologically active
central mediators have an important part to
free cortisol than plasma or serum (Kirschbaum
& Hellhammer, 1994). If low levels of cortisolwere to mediate the symptoms of CFS it wouldbe the free, unbound fraction that is important. STUDIES OF BASAL HPA AXIS
However, while Strickland et al. (1998) found
FUNCTION
significantly reduced cortisol from two morning
The strength of the first hypothesis has been
saliva samples, Wood et al. (1998), who took
tested by several studies that measured basal
16 samples throughout the day, found signifi-
cortisol in patients with CFS. These are sum-
cantly raised baseline cortisol, and Young et al.
marized in Table 1. Despite the early finding of
(1998) found no significant difference. Aside
low basal cortisol by Poteliakhoff (1981) and the
from the differences in the number and timing
NIH group (Demitrack et al. 1991), the majority
of saliva samples, characteristics of the study
of further studies have failed to replicate this.
samples may help to explain the inconsistent
Differences in methodology, and sample charac-
teristics may explain the variety of results. Methodology Sample confounds
Three basic methods of measuring baseline
One important confound is co-morbid depress-
cortisol have been employed : plasma, urine –
ive illness, present in approximately 50 % of
24 h urinary free cortisol (UFC) excretion – and
CFS patients. High circulating cortisol is a well
saliva. The majority of studies finding no
replicated finding in major depression (Dinan,
significant difference in baseline cortisol in
1994) and so presence of depression makes the
patients with CFS used plasma samples (Bearn
cortisol findings more difficul to interpret. et al. 1995 ; Yatham et al. 1995 ; Dinan et al.
Indeed, the subjects studied by Wood et al.
1997 ; Scott et al. 1998 a, b, c). Plasma samples
(1998) included five out of 10 subjects with high
entail intravenous cannulation in a hospital
Beck Depression Inventory scores (15–19). This
setting, both of which may induce a stress
may explain their unique finding of significantly
response, and a subsequent rise in circulating
raised baseline cortisol in their sample of CFS
cortisol. In addition, plasma samples measure
patients. Other studies have been inconsistent in
more than just the biologically active free cortisol
their exclusion of co-morbid psychiatric illness,
(Kirschbaum & Hellhammer, 1994). Three
and several do not even report data (see Table
1). Length of illness is another potential con-
measured UFC – a non-invasive method. The
founding factor, not always reported on (Table
Bart’s group (Scott & Dinan, 1998) and the
1). The original study by the NIH group used
King’s group (Cleare et al. 2001 a) replicated the
subjects with a particularly long illness (mean
finding of low basal cortisol, but Young et al.
7n2 years). Some groups who failed to replicate
(1998) found no significant difference. However,
their finding used subjects with considerably
despite the wide usage of UFC in depression
shorter illness duration (Wood et al. 1998 ;
research (Murphy, 1968 ; Stokes et al. 1984), a
Young et al. 1998). Few studies report on
controlled study of different cortisol measures
severity of the fatigue or disability, and there is
found it to be an unreliable indicator of HPA
reason to suggest that some behavioural conse-
activity (Thompson et al. 1992). Also, since
quences of fatigue may themselves cause the
free cortisol only represents 2–3 % of the cir-
shift in adrenocortical functioning observed by
culating cortisol metabolites (Raven & Taylor,
the NIH group (Demitrack et al. 1991). For
1996), a shift in the balance of cortisol metabolic
example Leese et al. (1996) found that short-
pathways could potentially affect the measured
UFC even in the presence of no change in total
changes observed in patients with CFS. They
conclude that the changes observed in CFS may
Summary of baseline studies of cortisol
CDC, Centers for Disease Control definition (Fukuda et al. 1994) ; NS l not significant ; Oxford, Oxford definition (Sharpe et al. 1991) ;
be secondary to disrupted sleep and social
thermore, several authors have noted (Sharpe et
routine, and thus an epiphenomenon in terms of
al. 1996) that basal values may not be the most
appropriate measure to determine HPA axis
Thus, the significance of basal cortisol levels
dysfunction, which leads us to consider the
in mediating fatigue is still not clarified. Fur-
by the Munich group (Heuser et al. 1994). This
CHALLENGE STUDIES
test is well validated and has been demonstrated
CRH challenge
to be of superior sensitivity compared to the
Measuring the response of the HPA axis to
challenge – pharmacological, physiological or
80 % v. 44 % ) for detecting HPA changes in
psychological, is arguably a better way to
depression (Deuschle et al. 1998).
investigate HPA dysfunction, since the HPA’srole is a dynamic one, in response to stress. The
ACTH challenge
first pharmacological challenge test in CFS was
by the NIH group, reported earlier. The Bart’s
suggested that there is up-regulation of ACTH
group (Scott et al. 1998 a) has recently repeated
receptors in the adrenal cortex of patients with
the CRH stimulation part of the NIH study, this
CFS (Demitrack et al. 1991). Further evidence
time in a sample of CFS patients without co-
for this comes from the Bart’s group (Scott et al.
morbid psychiatric disorder. They too found
1998 b) who measured cortisol responses to a
attenuated ACTH responses to exogenous ovine
low dose ACTH challenge test (1 µg). They
demonstrated an inverse relationship between
basal levels of ACTH, and on that evidence
the baseline cortisol and the incremental cortisol
ruled out underfunctioning pituitary cortico-
rise in response to ACTH, again suggesting
trophs being responsible for the poor ACTH
hypersensitivity of the adrenal cortex to ACTH
in CFS subjects with impaired HPA activity.
normal in the Bart’s sample, and they suggest
They also found significantly attenuated cortisol
desensitization of CRH receptors on the pitu-
responses overall, which they interpret as re-
itary corticotrophs as a possible explanation.
flecting a diminished adrenocortical reserve
Such an explanation would not be consistent
with the theory of decreased hypothalamic CRH,
ACTH, in line with the NIH group’s interpret-
since then up-regulation of CRH receptors
ation of their data. The results from both groups
would predict adrenal cortical atrophy, and a
responses to exogenous CRH. To reconcile these
recent study from the Bart’s group has found
contrasting theories, the Bart’s group suggest
preliminary evidence for this in a group of eight
that CFS is a stress-related disorder. They
CFS subjects, using computerized tomography
hypothesize first, that initial stress may cause an
(Scott et al. 1999 a). However, since subjects
elevation in CRH with consequent down-regu-
were chosen specifically to have a blunted
cortisol response to ACTH, the authors admit
corticotrophs. Secondly, they hypothesize that
that this may not generalize to all CFS subjects ;
this down-regulation may fail to normalize
indeed, it is possible that normals selected for
following reduction in CRH levels. This would
low cortisol responses would also show smaller
be an example of abnormal plasticity in the
CRH receptor which could be investigated by
Recent work from the King’s group attempted
studying pituitary–adrenal activation by CRH,
to replicate the results of low dose ACTH
during and following recovery from CFS. This
challenge in 20 non-depressed, medication-free
would also provide evidence on whether the
CFS subjects. The authors found no difference
HPA axis abnormalities are a state- or trait-
in cortisol response in comparison to a matched
dependent phenomenon (Scott et al. 1998 a).
control group, though in males there was a trend
What might give rise to such abnormal func-
towards a blunted response (Hudson & Cleare,
tioning of the CRH receptor is far from clear.
The differing basal levels of ACTH between thetwo groups may also be due to the inherent
5-HT agonist challenge (see Table 2)
difficulties of measuring this pulsatile hormone,
In the pathophysiology of depression, the re-
lationship between the hypercortisolaemia and
A further challenge test, which may help to
5-HT may be important (Cleare et al. 1996 ;
clarify the state of the HPA in CFS, is the
Dinan, 1996 ; McAllister-Williams & Young,
combined dexamethasone\CRH test pioneered
1998). Glucocorticoids have been demonstrated
Summary of studies of 5-HT agonist challenge
changes in dopamine function, ratherthan 5-HT
CFS, may explain fatigue or besecondary to behavioural changes
CDC, Centers for Disease Control definition (Fukuda et al. 1994) ; PVFS, Post-viral fatigue syndrome ; Oxford, Oxford definition (Sharpe et al. 1991).
to exert an inhibitory effect on central 5-HT
for increased 5-HT function in CFS, it also
neurotransmitter function (De Kloet et al. 1986 ;
suggests that HPA and 5-HT function may be
McAllister-Williams et al. 1998), while on the
pathologically altered in opposite directions in
other hand, stress-induced CRH secretion is
the two conditions. The King’s group also note
modulated by 5-HT (Delbende et al. 1992 ;
that in depression, the neurochemical changes
Dinan, 1996). Accumulating evidence, from the
are associated with insomnia, anorexia and
use of 5-HT agonists, now suggests that 5-HT
agitation, whereas the opposite chemical changes
neurotransmission may be altered in CFS. 5-HT
in CFS are associated with the reverse of these
pathways from the dorsal raphe nuclei to the
paraventricular nucleus of the hypothalamus are
While some have replicated the finding of
thought to bring about the secretion of hypotha-
enhanced prolactin response to -fenfluramine
lamic–pituitary releasing peptides involved in
(Sharpe et al. 1997), others have not (Bearn et al.
the release of prolactin and ACTH from the
1995 ; Yatham et al. 1995). Methodological
anterior pituitary (Checkley, 1980). Therefore,
measuring serial prolactin and cortisol responses
inconsistencies. Bearn et al.’s sample had poor
to 5-HT agonist drugs are thought to reflect
age and gender matching, and Yatham et al.’s
hypothalamic-5-HT neurotransmitter function.
subjects had a heterogeneous psychiatric history.
Several different 5-HT agonists have been
Also, Yatham et al. used ,-fenfluramine
used. Bakheit et al. (1992) measured the prolactin
instead of -fenfluramine. The former includes
response to the 5-HT" receptor agonist bus- both stereoisomers and has less specific neuro-
pirone, and found it to be significantly raised in
chemical effects, including additional catechol-
CFS subjects compared with controls, suggesting
up-regulation of post-synaptic 5-HT" receptors
Further evidence for disturbed functioning of
in the hypothalamus. However, buspirone also
the 5-HT and HPA axis relationship comes from
binds to dopamine D2 receptors, and so its
a study by the Bart’s group (Dinan et al. 1997),
ability to increase prolactin may be mediated in
who used ipsapirone – a partial agonist of 5-
part by D2 receptor blockade (Meltzer et al.
HT" receptors, like buspirone, but without
1991 ; Maskall et al. 1995). Sharpe et al. (1996)
action at dopamine receptors. They were testing
tested this by measuring growth hormone re-
the hypothesis that in CFS, abnormalities of
sponses in addition to prolactin, since it is
HPA function arise from disturbance in sero-
known that GH release is much more likely to
tonergic (5-HT) inputs. In healthy controls
be mediated via 5-HT" receptors (Cowen, 1993). ACTH and cortisol rise in a dose-dependent
While prolactin was significantly increased in
fashion on stimulation with ipsapirone, though
CFS subjects, GH was not, suggesting that the
in CFS patients they found significantly attenu-
enhanced prolactin response may be due to
abnormalities in dopamine neurotransmission,
responses. This finding could be interpreted as
evidence of decreased responsivity of 5-HT"A
receptors at the hypothalamic level. However,
selective 5-HT-releasing agent -fenfluramine.
other interpretations such as either decreased
The King’s group (Cleare et al. 1995) measured
responsivity of CRH receptors on the pituitary
prolactin and cortisol responses to -fenflura-
corticotrophs, or underactivity of the pituitary
corticotrophs are possible which do not necess-
healthy controls, and patients with major de-
arily invoke abnormalities of the 5-HT system.
pression. Relative to controls, prolactin respon-
As noted earlier, the Bart’s group (Scott et al.
ses were significantly higher in CFS patients,
1998 a) have already suggested decreased re-
and significantly lower in those with major de-
sponsivity of CRH receptors on the pituitary
pression. In addition, prolactin responses were
corticotroph to explain the attenuated ACTH
found to be inversely proportional to the baseline
response to exogenous CRH stimulation, found
cortisol. Thus, CFS patients had low baseline
cortisol and enhanced prolactin response to -
although the Bart’s group found significantly
fenfluramine, and depressed subjects the con-
attenuated 5-HT" mediated ACTH responses
verse. Not only does this study provide evidence
to ipsapirone, the site of abnormality (5-HT"A
receptor, CRH receptor or pituitary cortico-
Indeed, Conti et al. (1998) have found decreased
β-endorphin levels in patients with CFS. Further
investigation of the opioid system is now
probes used in CFS are perfect. As well as the
indicated, including measures of the other
problems of selectivity for the 5-HT system and
endogenous opioids, and investigation of the
its many receptor subtypes, most studies do not
endogenous opioid receptor ligands. Future
measure plasma levels of the probes or take into
studies should include objective measures of
account active metabolites. These problems
physical activity, since activity levels may affect
could potentially account for the inconsistencies
opioid tone (Inder et al. 1995).
in the 5-HT challenge tests reported in CFS. Argenine vasopressin Naloxone challenge
Another hormone exerting control over the
Several other neurotransmitters are also being
HPA is argenine vasopressin (AVP), which acts
implicated in CFS, such as the opioidergic
system, which unlike the stimulatory 5-HT
release (Lamberts et al. 1984 ; Antoni, 1993).
system, exerts a predominantly inhibitory influ-
Therefore a deficit in endogenous AVP could
ence upon the HPA axis in man (Taylor et al.
contribute towards the attenuated ACTH re-
1983). The Bart’s group (Scott et al. 1998 c) put
sponse seen with exogenous CRH stimulation.
forward the hypothesis that the documented
Indeed, Bakheit et al. (1993) found basal levels
down regulation of the HPA axis in CFS may be
of AVP to be significantly reduced in response to
secondary to increased opioidergic tone. They
water deprivation challenge in CFS patients.
stimulated CFS patients and controls with the
The Bart’s group (Scott et al. 1999 b) found that
opiate receptor antagonist, naloxone. In healthy
desmopressin, a vasopressin analogue, was able
subjects naloxone will decrease central opio-
to normalize the blunted ACTH response to
idergic tone, thereby releasing the HPA axis
from inhibitory control, and causing a rise in
hypothesized that this was due to upregulated
ACTH and cortisol. They found that in CFS
AVP receptors on the pituitary, again consistent
patients compared to controls there was an
attenuated ACTH response to naloxone. Theyconclude that this effectively rules out increased
CIRCADIAN RHYTHMS
opioidergic tone as a cogent explanation for theabnormal HPA function in CFS – the opposite
In contrast to the many studies observing
finding to that which they predicted. However,
neuroendocrine function at one time point, there
their conclusion may be inaccurate due to the
have been relatively few studies of diurnal
difficulty of interpreting challenge tests using a
variation, or circadian rhythm. MacHale et al.
receptor antagonist as the probe. The outcome
(1998) demonstrated a significantly attenuated
will depend upon receptor affinities of the probe
diurnal variation of serum cortisol in CFS,
compared with endogenous opioids, and relative
though the absolute concentrations at each time
changes in receptor occupancies. The balance of
point were not significantly different compared
these factors may theoretically determine quite
to controls. However, the relevance of diurnal
different outcomes from the naloxone challenge.
variation is highlighted by their additional
This issue warrants further detailed study.
observation of a significant relationship between
If however, the Bart’s group is correct in their
the degree of diurnal variation in cortisol and
interpretation of decreased opioidergic tone in
measures of functional improvement over the
CFS, then it is interesting considering that pain
past year and current social functioning. Loss of
prone individuals have been found to have lower
diurnal variation in cortisol has previously been
than normal concentrations of opiates in the
demonstrated in fibromyalgia, pain syndromes
CSF (Terenius & Wahlstrom, 1978). Thus, the
and depressive illness (Lascelles et al. 1974 ;
Bart’s group suggest that a reduction in en-
Carroll et al. 1976 ; McCain & Tilbe, 1989), all
dogenous opioid tone may explain the common
of which have significant symptom overlap with
pain symptoms which CFS patients experience,
CFS. Supporting McHale et al. (1998), a
such as myalgia, arthralgia and headaches.
significant decrease in the early morning surge
dopoulos et al. 1997), although other studies
directions. The HPA-stress axis and the growth
have found no significant difference in the
hormone (GH) axis do interact with one another,
circadian rhythm of cortisol (Raciatti et al.
as demonstrated, for example, by blunted growth
1998 ; Wood et al. 1998 ; Young et al. 1998).
following prolonged stress in childhood. How-ever, a different observation led to the first GHstudy in fibromyalgia. In 1975 Moldofsky et al. FIBROMYALGIA
demonstrated a distinct disturbance of stage-4,
Fibromyalgia is a condition characterized by
non-REM sleep in patients with fibromyalgia,
widespread muscle pain, fatigue and sleep
characterized by alpha-wave intrusion into the
disturbances. Most authors agree that the
delta rhythm. They also induced a transient
symptomatology of fibromyalgia overlaps with
syndrome similar to fibromyalgia by depriving
CFS, and some now believe that it is essentially
healthy subjects of this stage of sleep. Stage-4
the same condition (Wessely et al. 1999). Of
sleep is closely related to the pulsatile secretion
particular interest are the findings from neuro-
of GH, and approximately 80 % of the total
endocrine studies, which on some, but not all,
daily production of GH is secreted during this
parameters show remarkable similarities to those
stage. GH regulates the hepatic production and
in CFS. At least two groups have demonstrated
release of somatomedin C (IGF-1) which is an
reduced 24 h urinary free-cortisol in patients
important mediator of muscle homeostasis and
with fibromyalgia (McCain & Tilbe, 1989 ;
repair, a deficiency of which would predispose to
Crofford et al. 1994). Furthermore, in response
muscle microtrauma and pain. This led Bennett
to exhaustive physical exercise, Van Denderen etet al. (1992) to hypothesize that disruption of
al. (1992) reported reduced adrenocortical ac-
stage-4 sleep in fibromyalgia would lead to low
tivation, and in response to exogenous CRH,
levels of IGF-1, and indeed their study confirmed
Griep et al. (1993) demonstrated a blunted
cortisol response. In contrast to CFS, both
Crofford et al. (1994) and Griep et al. (1993,
have been demonstrated in CFS by two groups
1998) found exaggerated ACTH responses to
(Allain et al. 1997 ; Berwaerts et al. 1998),
CRH stimulation. The reason for this divergence
although not by another (Bennett et al. 1997).
is not clear, though Demitrack (1997) suggests
The study by Allain et al. (1997) also demon-
that a clue may come from AVP levels. Whereas
strated a reduced GH response to insulin-
induced hypoglycaemia, though Berwaerts et al.
(Bakheit et al. 1993), in fibromyalgia they were
(1998) failed to repeat this. In an attempt to
found to be high compared to controls, in
clear away the confusion from inconsistent
response to postural challenge. Since AVP acts
results, the King’s group (Cleare et al. 2000)
carried out the largest and most comprehensive
difference in AVP levels would be consistent
study of the GH axis to date in patients with
with the differences demonstrated in ACTH
CFS closely matched to healthy controls. They
failed to find any significant differences in either
Thus, comparison of CFS with fibromyalgia
baseline or challenge tests of GH function, and
highlights both similarities and differences in
concluded that there is no evidence for GH
neuroendocrinology. It may be that the dif-
deficiency in CFS patients free from co-morbid
ferences reflect distinct pathophysiologies for
the two syndromes. However, the similarities,both in reduced HPA activation, symptoma-tology and abrupt stress-related onset suggest
TREATMENT STUDIES
Several treatment studies have attempted toreverse the symptoms of CFS and fibromyalgia
GROWTH HORMONE, CFS AND
by artificially replacing hormones thought to be
FIBROMYALGIA
deficient in these conditions. Such studies serve
The rationale for studying growth hormone in
the dual purposes of : (1) testing new logical
therapeutic strategies ; and (2) further testing the
in dietary salt intake. The aim had been to
hypothesis that symptoms are due to disordered
suppress the supposed reflex underlying neurally
mediated hypotension by increasing blood vol-
In fibromyalgia, Bennett and colleagues fol-
lowed up their earlier finding of low somato-
However, two further trials, this time using
medin C (IGF-1) levels in 30 % of patients, by
hydrocortisone, were able to show significant
conducting a randomized, double-blind, con-
improvements in patients with CFS. McKenzie
trolled trial of growth hormone replacement
et al. (1998) used a dosing regime chosen to
(Bennett et al. 1998). They included only those
approximate the normal diurnal variation in
patients who had low levels of the growth
cortisol (20–30 mg at 8 a.m., and 5 mg at 2 p.m.,
medin C). Daily subcutaneous GH injections
significant benefit on a global health scale,
resulted in a prompt and sustained increase in
though not on other scales. The cost of this mild
IGF-1 levels, and at 9 months, a significant
improvement was significant adrenal suppres-
overall improvement in symptomatology and
sion in 12 out of 33 patients, which led the
number of tender points. The authors conclude
authors to advise against the use of hydro-
that although the high cost-benefit ratio pre-
cortisone in clinical practice. The King’s group
cludes its therapeutic use in fibromyalgia
(Cleare et al. 1999) also reported a randomized,
patients, the study provides further support for
controlled trial of hydrocortisone in CFS.
the theory that a secondary growth hormone
deficiency is responsible for some of their
5–10 mg, which are consistent with replacement
of the reduction in cortisol output of between
Moorkens et al. (1998) carried out a similar,
30–40 % in CFS, reported in some studies
though smaller, randomized controlled trial of
(Demitrack et al. 1991 ; Scott & Dinan, 1998). In
contrast to McKenzie et al. study, no significant
selected patients with a demonstrated deficiency
adrenal suppression was seen, and there were no
of GH, though their results were less marked.
other serious adverse effects. There was a
There was no improvement in quality of life,
clinically significant fall in fatigue scores in 34 %
after 12 months, although 4 out of 17 patients
on active treatment, compared with 13 % on
were able to return to work after prolonged sick
placebo, and this benefit declined rapidly on
leave. The lack of any clear benefit in patients
crossover to placebo treatment. In those whose
with CFS is perhaps not surprising following the
fatigue improved, physical role limitations were
extensive study of the GH axis by the King’s
also significantly improved, as were mean dis-
group (Cleare et al. 2000), noted above.
ability scores. Although pre-treatment endocrine
Of interest to the hypothesis of low circulating
disturbance did not predict response to hy-
glucocorticoids as the mediator of symptoms in
drocortisone, those that did respond showed
CFS, are three recent randomized controlled
normalization of the cortisol response to CRH
trials of steroid replacement therapy. The first
challenge, whereas non-responders did not
was by Peterson et al. (1998), who used low-
(Cleare, 2001 b). Overall, this lends support to
doses (0n1–0n2 mg) of the mineralocorticoid
the suggestion that HPA axis disturbance may
fludrocortisone. They found no improvement on
be one reversible factor contributing to fatigue
any symptom or test of function, over 6 weeks,
in CFS. Despite this, the authors warn against
between active drug and placebo groups. Their
simple acceptance that normalization of the
rationale for treating with fludrocortisone was
HPA axis is a direct effect of hydrocortisone, as
unconnected with the neuroendocrine hypoth-
clinical improvement leads to a complex of
eses presented here. Their study followed the
changes in sleep, exercise, mood and circadian
demonstration by Bou-Holaigh et al. (1995) that
rhythms (above, and Cleare, 2001 b). Clearly,
CFS is associated with neurally mediated hy-
further evaluation is needed of hydrocortisone
potension. Bou-Holaigh et al. also noted in an
as a possible treatment in some patients with
uncontrolled study, that some CFS patients
CFS, and further study of the HPA axis in those
responding to non-pharmacological treatments
treatment with fludrocortisone and an increase
such as graded exercise or cognitive–behavioural
therapy, both of which are effective in CFS
SUMMARY AND CONCLUSIONS
Anti-depressants have also been tried in the
treatment of CFS – the rationale being the
1991 suggested three related theories for the
overlap in symptoms between depressed, and
mediation of symptoms in CFS (Demitrack et
chronic fatigue patients, and the suggestion that
al. 1991). First, that the fatigue is due directly to
CFS may be a variant form of depression.
low circulating cortisol ; secondly that it is due to
However, the neuroendocrine studies of the
abnormalities of central neurotransmitters in-
HPA axis reviewed above, demonstrate marked
volved in HPA axis function (e.g. CRH) ; and
differences between the two conditions, suggest-
thirdly that symptoms are a result of a more
ing different pathophysiologies (Cleare et al.
complex disturbance of the relationship between
1995 ; Scott & Dinan, 1998 ; Strickland et al.
the two. Support for all three hypotheses has
1998). In further support of distinct pathologies,
been found, though it has been problematical
is the randomized controlled trial of fluoxetine
providing consistent evidence, and attempts to
in CFS reported by Vercoulen et al. (1996). On
make causal attributions require caution on the
a range of measures, including subjective fatigue,
available evidence. On balance, there does
depression, well-being, functional impairment
appear to be down-regulation of the HPA axis
and activity, they found no beneficial effect for
in at least some patients with CFS, and that this
fluoxetine. Even those CFS patients with co-
is most apparent on challenge tests, rather than
morbid depression showed no improvement in
measures of baseline function. This would
mood, suggesting that dysphoria in CFS may
concur with patients’ reports of symptoms
have a different basis to that in primary major
worsening following physical or emotional stress
depression. Three further trials using mono-
amine oxidase inhibitors (MAOIs) to treat CFS
In keeping with the first hypothesis, reduced
have been carried out. Natelson et al. (1996)
circulating cortisol may also explain the modest,
used a low-dose of the non-specific MAOI,
non-specific activation of immune responses
phenelzine, in a double-blind, randomized con-
reported in CFS (Wessely et al. 1998), since
trolled trial. They found a very small, though
glucocorticoids usually dampen immune acti-
statistically significant improvement, which was
vation. Several studies have supported the role
independent of any anti-depressant effect. They
followed this up with a single-blind, placebo
(Bakheit et al. 1992 ; Demitrack et al. 1992 ;
phase-in trial of the specific MAO B receptor
Cleare et al. 1995 ; Sharpe et al. 1996, 1997). In
inhibitor selegiline (Natelson et al. 1998), again
particular, a deficiency of hypothalamically
finding a small, but significant benefit, in the
derived CRH is an attractive hypothesis con-
absence of any anti-depressant effect. The most
sidering that central administration of this
recent study found the strongest effect seen to
neurohormone to animals produces marked be-
date, comparing 450–600 mg of moclobemide
havioural and locomotor activation (Britton et
to placebo over 6 weeks (Hickie et al. 2000). al. 1982 ; Sutton et al. 1982 ; Swerdlow et al.
Significant subjective global improvement was
1986). The possibility of the third, complex, but
reported in 24\47 patients on active treatment
vaguer hypothesis serves to illustrate our current
(51 %) compared to 14\43 on placebo (33 %).
ignorance of how any such chemical changes
There was a significant and progressive improve-
may translate into subjective symptoms.
ment in ratings of ‘ vigour ’, though the re-
duction in disability over the short treatment
dysregulated in CFS, it is far from clear how the
period was not significantly greater than that
two relate causally. Leese et al. (1996) provided
seen with placebo. Interestingly, improvement
evidence that the HPA changes may be sec-
was seen equally in those with and without co-
ondary to behavioural change, whilst the King’s
morbid depression, while the largest response
group (Cleare et al. 2001 b) have demonstrated
sizes were seen in a subgroup with immuno-
that symptomatic improvement is associated
logical changes. Once again, these studies suggest
with a reversal of the endocrine changes. Down-
a rather different pattern of antidepressant
regulation of the HPA axis is still weak as an
response to that seen in classical depression.
aetiological theory since no theoretical model
exists of how this may come about – from
fenfluramine and insulin-induced hypoglycaemia in chronic fatigue
viruses, stress or other insult. This is in contrast
syndrome. Biological Psychiatry 37, 245–252.
Bennett, A. L., Mayes, D. M., Fagioli, L. R., Guerriero, R. &
to depression, where a robust model exists of
Komaroff, A. L. (1997). Somatomedin C (insulin-like growth
how chronic psychological stress leads to up-
factor I) levels in patients with chronic fatigue syndrome. Journal of Psychiatric Research 31, 91–96.
Bennett, R. M., Clark, S., Campbell, S. & Burckhardt, C. (1992).
Low levels of somatomedin C in patients with fibromyalgia.
(Checkley, 1996). The finding by White et al. Arthritis and Rheumatism 35, 1113–1116.
Bennett, R. M., Clark, S. & Walczyk, J. (1998). A randomized
(1998) that following glandular fever, 9–22 % of
double-blind, placebo-controlled study of growth hormone in the
subjects develop CFS, suggests that new cases of
treatment of fibromyalgia. American Journal of Medicine 104,
glandular fever may represent a useful starting
Berwaerts, J., Moorkens, G. & Abs, R. (1998). Secretion of growth
point for future longitudinal studies of neuro-
hormone in patients with chronic fatigue syndrome. Growth
endocrine function. Such an approach may help
hormone and IGF Research 8 (SB), 127–129.
establish whether under-activity in the HPA axis
Bou-Holaigah, I., Rowe, P. C., Kan, J. & Calkins, H. (1995). The
relationship between neurally mediated hypotension and the
is a trait\vulnerability factor or a state factor,
chronic fatigue syndrome. Journal of the American Medical
and whether it is secondary to a change in
Association 274, 961–967.
Britton, D., Koob, G., Rivier, J. & Vale, W. (1982). Intraventricular
behaviour, such as prolonged rest or altered
corticotrophin-releasing factor enhances behavioural effects of
sleep patterns. Correlating the development of
novelty. Life Sciences 31, 363–367.
HPA dysfunction over time with the devel-
Buchwald, D., Sullivan, J. L. & Komaroff, A. L. (1987). Frequency
of ‘ chronic active Epstein-Barr virus infection ’ in a general
opment of CFS, would clearly lend support to a
medical practice. Journal of the American Medical Association 257,
role for HPA dysfunction in the aetiological
Carroll, B., Curtis, G. & Mendels, J. (1976). Neuroendocrine
regulation in depression. I : Limbc system-adrenocortical dys-
Although in depression, HPA axis overdrive
function. Archives of General Psychiatry 33, 1039–1044.
is well established, no intervention directly
Chaouloff, F. (1993). Physiopharmacological interactions between
stress hormones and central serotonergic systems. Brain Research
targeting this dysfunction has yet proven to be
Reviews 18, 1–32.
clinically useful and safe. However, in CFS,
Checkley, S. A. (1980). Neuroendocrine tests of monoamine function
where antidepressants have been disappointing
in man : a review of basic theory and its application to the study of depressive illness. Psychological Medicine 10, 35–53.
(Vercoulen et al. 1996), direct manipulation of
Checkley, S. A. (1996). The neuroendocrinology of depression and of
the HPA axis, with oral hydrocortisone, has
chronic stress. British Medical Bulletin 52, 597–617.
shown promising results (Cleare et al. 1999).
Cleare, A. J., Bearn, J., Allain, T., McGregor, A., Wessely, S.,
Murray, R. & O ’Keane, V. (1995). Contrasting neuroendocrine
This requires further evaluation, particularly in
response in depression and chronic fatigue syndrome. Journal of
larger, less selected samples to establish efficacy,
Affective Disorders 35, 283–289.
tolerability and safety, before it can be recom-
Cleare, A. J., Murray, R. M. & O ’Keane, V. (1996). Reduced
prolactin and cortisol responses to -fenfluramine in depressed
compared to healthy matched control subjects. Neuropsycho- pharmacology 14, 349–354.
Cleare, A. J., Heap, E., Malhi, G. S., Wessely, S., O’Keane, V. &
REFERENCES
Miell, J. (1999). Low-dose hydrocortisone in chronic fatigue syndrome : a randomised crossover trial. Lancet 353, 455–458.
Allain, T. J., Bearn, J. A., Coskeran, P., Jones, J., Checkley, A.,
Cleare, A. J., Sookdeo, S. S., Jones, J., O ’Keane, V. & Miell, J.
Butler, J., Wessely, S. & Miell, J. P. (1997). Changes in growth
(2000). Integrity of the GH\IGF system is maintained in patients
hormone, insulin, insulin-like growth factors (IGFS), and IGF-
with chronic fatigue syndrome. Journal of Clinical Endocrinology
binding protein-1 in chronic fatigue syndrome. Biological Psy-
and Metabolism 85, 1433–1439. chiatry 41, 567–573.
Cleare, A. J., Blair, D., Chambers, S. & Wessely, S. (2001 a). Urinary
Antoni, F. (1993). Vasopressinergic control of pituitary adeno-
free cortisol in chronic fatigue syndrome. American Journal of
corticotrophin secretion comes of age. Frontiers in Neuroendo-
Psychiatry 158, 641–643. crinology 14, 76–122.
Cleare, A. J., Miell, J., Heap, E., Sookdeo, S., Young, L., Malhi,
Bakheit, A., Behan, P., Dinan, T., Gray, C. & O’Keane, V. (1992).
G. S. & O’Keane, V. (2001 b). Hypothalamo–pituitary–adrenal
Possible upregulation of hypothalamic 5-hydroxytryptamine re-
axis dysfunction in chronic fatigue syndrome, and the effects of
ceptors in patients with postviral fatigue syndrome. British Medical
low-dose hydrocortisone therapy. Journal of Clinical EndocrinologyJournal 304, 1010–1012. and Metabolism 86, 3545–3554.
Bakheit, A., Behan, P., Watson, W. & Morton, J. (1993). Abnormal
Conti, F., Pittoni, V., Sacerdote, P., Priori, R., Meroni, P. L. &
arginine-vasopressin secretion and water metabolism in patients
Valesi, G. (1988). Decreased immunoreactive beta-endorphin in
with postviral fatigue syndrome. Acta Neurologica Scandinavica
mononuclear leucocytes from patients with chronic fatigue
87, 234–238.
syndrome. Clinical and Experimental Rheumatology 16, 729–732.
Baxter, J. D. & Tyrel, J. B. (1981). The adrenal cortex. In
Cowen, P. (1993). Serotonin receptor subtypes in depression : evidence
Endocrinology and Metabolism (ed. P. Felig, J. D. Baxter, A. E.
from studies in neuroendocrine regulation. Clinical Neuropharma-
Broadus and L. A. Frohman), pp. 385–510. McGraw-Hill : New
cology 16 (suppl. 3), S6–S18.
Crofford, L., Pillemer, S., Kalogeras, K., Cash, J. M., Michelson, D.,
Bearn, J., Allain, T., Coskeran, P., Munro, N., Butler, J., McGregor,
Kling, M. A., Sternberg, E. M., Gold, P. W., Chrousos, G. P. &
A. & Wessely, S. (1995). Neuroendocrine response to -
Wilder, R. L. (1994). Hypothalamic–pituitary–adrenal axis per-
turbations in patients with fibromyalgia. Arthritis and Rheumatism
Inder, W., Ellis, M., Evans, M. & Donald, R. (1995). A comparison
37, 1583–1592.
of the naloxone test with ovine CRH and insulin hypoglycaemia in
David, A. S. (1991). Postviral fatigue syndrome and psychiatry.
the evaluation of the hypothalamic–pituitary–adrenal axis : in-
British Medical Bulletin 47, 966–988.
teraction with endogenous opioid peptides. Clinical Endocrinology
De Kloet, E., Sybesma, H. & Reul, J. (1986). Selective control by
43, 283–290.
corticosterone of serotonin-1 receptors capacity in raphe–
Kertesz, G., Bourcier, B., Cailla, H. & Jean, F, (1998). Immuno-
hippocampal system. Neuroendocrinology 42, 513–521.
radiometric assay of succinylated corticotrophin : an improved
Delbende, C., Delarue, C., Lefebre, H., Bunel, D., Szafarczyk, A.,
method for quantification of ACTH. Clinical Chemistry 44, 78–85.
Mocaer, E., Kamoun, A., Jegou, S. & Vaudry, H. (1992).
Kirschbaum, C. & Hellhammer, D. H. (1994). Salivary cortisol in
Glucocorticoids, transmitters and stress. British Journal of Psy-
psychoneuroendocrine research : recent developments and appli-
chiatry 160 (suppl.), 24–34.
cations. Psychoneuroendocrinology 19, 313–333.
Demitrack, M. A. (1997). Neuroendocrine correlates of chronic
Lamberts, S., Verleun, S., Oosteron, R., DeJong, F. & Hackeng, W.
fatigue syndrome : a brief review. Journal of Psychiatric Research
(1984). Corticotrophin-releasing factor (ovine) and vasopressin
31, 69–82.
exert a synergistic effect on adrenocorticotrophin release in man.
Demitrack, M., Dale, J., Straus, S., Lawe, L., Listwak, S. J., Kruesi,
Journal of Clinical Endocrinology and Metabolism 58, 298–303.
M. J., Chrousos, G. P. & Gold, P. W. (1991). Evidence for
Lascelles, P., Evans, P., Mersky, H. & Sabur, M. (1974). Plasma
impaired activation of the hypothalamic–pituitary–adrenal axis in
cortisol in psychiatric and neurological patients with pain. Brain
patients with chronic fatigue syndrome. Journal of Clinical97, 533–538. Endocrinology and Metabolism 73, 1224–1234.
Leese, G., Chattington, P., Fraser, W., Vora, J., Edwards, R. &
Deuschle, M., Schweiger, U., Gotthardt, U., Weber, B., Korner, A.,
Williams, G. (1996). Short-term night-shift working mimics the
Schmider, J., Stanhardt, H., Lammers, C. H., Krumm, B. &
pituitary–adrenocortical dysfunction of chronic fatigue syndrome.
Heuser, I. (1998). The combined dexamethasone\cortocotrophin-
Journal of Clinical Endocrinology and Metabolism 81, 1867–1870.
releasing hormone stimulation test is more closely associated with
Lesch, K. P., Mayer, S., Disselkamp-Tietze, J., Hoh, A., Schoelln-
features of diurnal activity of the hypothalamic–pituitary–
hammer, G. & Schulte, H. M. (1990). Sub-sensitivity of the 5-
adrenocortical system than the dexamethasone test. BiologicalPsychiatry 43, 762–766.
response to ipsapirone in unipolar depression. Life Sciences 46,
Dinan, T. G. (1994). Glucocorticoids and the genesis of depressive
illness. A psychobiological model. British Journal of Psychiatry
McAllister-Williams, R. H. & Young, A. H. (1998). The patho-
164, 365–371.
physiology of depression : a synthesis of the role of serotonin and
Dinan, T. G. (1996). Serotonin and the regulation of hypothalamic–
cortocosteroids. In New Models for Depression. Advances in
pituitary–adrenal axis function. Life Sciences 58, 1683–1694. Biological Psychiatry, vol. 19 (ed. D. Ebert and K. P. Ebmeier), pp.
Dinan, T. G., Majeed, T., Lavelle, E., Scott, L. V., Berti, C. & Behan,
P. (1997). Blunted serotonin-mediated activation of the hypotha-
McAllister-Williams, R. H., Ferrier, I. N. & Young, A. H. (1998).
lamic–pituitary–adrenal axis in chronic fatigue syndrome. Psycho-
Mood and neuropsychological function in depression : the role of
neuroendocrinology 22, 261–267.
corticosteroids and serotonin. Psychological Medicine 28, 573–584.
Fleshner, M., Deak, T., Spencer, R. L., Laudenslager, M. L.,
McCain, G. & Tilbe, K. (1989). Diurnal hormone variation in
Watkins, L. R. & Maier, S. F. (1995). A long term increase in basal
fibromyalgia : a comparison with rheumatoid arthritis. Journal of
levels of corticosterone and a decrease in corticosteroid-binding
Rheumatology 16 (suppl.), 154–157.
globulin after acute stressor exposure. Endocrinology 136, 5336–
MacHale, S. M., Cavanagh, J. T. O. & Lawrie, S. M. (1998). Diurnal
variation of adrenocortical activity in chronic fatigue syndrome.
Fukuda, K., Strauss, S., Hickie, I., Sharpe, M., Dobbins, J. &
Neuropsychobiology 38, 213.
Komaroff, A. (1994). The chronic fatigue syndrome : a com-
McKenzie, R., O’Fallon, A., Dale, J., Demitrack, M., Sharma, G.,
prehensive approach to its definition and study. Annal of InternalMedicine
Deloria, M., Garcia-Borreguero, D., Blackwelder, W. & Straus, S. 121, 953–959.
Gala, R. R. & Westphal, U. (1966). Further studies of the
(1998). Low-dose hydrocortisone for treatment of chronic fatigue
corticosteroid-binding globulin in the rat : proposed endocrine
syndrome : a randomized controlled trial. Journal of the American
control. Endocrinology 79, 67–76. Medical Association 280, 1061–1066.
Griep, E., Boersma, J. & De Kloet, E. (1993). Altered reactivity of the
Maskall, D. D., Zis, A. P., Lam, R. W., Clark, C. M. & Kuan, A. J.
hypothalamic-pituitary-adrenal axis in the primary fibromyalgia
(1995). Prolactin response to buspirone challenge in the presence of
syndrome. Journal of Rhuematology 20, 469–474.
dopaminergic blockade. Biological Psychiatry 38, 235–239.
Griep, E. N., Boersma, J. W., Lentjes, E. G., Prins, A. P., van der
Meltzer, H., Gudelsky, G., Lowy, M., Nash, J. & Koenig, J. (1991).
Korst, J. K. & de Kloet, E. R. (1998). Function of the hypothal-
Neuroendocrine effects of buspirone : mediation by dopaminergic
amic–pituitary–adrenal axis in patients with fibromyalgia and low
and serotonergic mechanisms. In Buspirone : Mechanisms and
back pain. Journal of Rheumatology 25, 1374–1381. Clinical Aspects (ed. G. Tunnicliff, A. S. Elison and O. P. Taylor),
Heuser, I., Yassouridis, A. & Holsboer, F. (1994). The combined
pp. 177–192. Academic Press : San Diego, CA.
dexamethasone\CRH test: a refined laboratory test for psychiatric
Moldofsky, H., Scarisbrick, P., England, R. & Smythe, H. (1975).
disorders. Journal of Psychiatric Research 28, 341–356.
Musculoskeletal symptoms and non-REM sleep disturbance in
Hickie, I. B., Wilson, A. J., Wright, J. M., Bennett, B. K., Wakefield,
patients with ‘ fibrositis syndrome ’ and healthy subjects. Psycho-
D. & Lloyd, A. R. (2000). A randomized, double-blind, placebo-
somatic Medicine 37, 241–351.
controlled trial of moclobemide in patients with chronic fatigue
Moorkens, G., Wynants, H. & Abs, R. (1998). Effect of growth
syndrome. Journal of Clinical Psychiatry 61, 643–648.
hormone treatment in patients with chronic fatigue syndrome.
Holmes, G., Kaplan, J., Stewart, J., Hunt, B., Pinsky, P. &
Growth Hormone and IGF Research 8 (suppl. B), 131–133.
Schnonberger, L. (1987). A cluster of patients with a chronic
Murphy, B. E. P. (1968). Clinical evaluations of urinary cortisol
mononeucleosis-like syndrome : is Epstein–Barr virus the cause ?
determination by competitive protein-binding radioassay. JournalJournal of the American Medical Association 257, 2297–2302. of Clinical Endocrinolology and Metabolism 28, 343–348.
Horwitz, C., Henle, W., Henle, G., Rudnick, H. & Latts, E. (1985).
Natelson, B. H., Cheu, J., Pareja, J., Ellis, S. P., Policastro, T. &
Long-term serological follow-up of patients with Epstein–Barr
Findley, T. W. (1996). Randomized, double-blind, placebo-phase
virus after recovery from infectious mononucleosis. Journal of
in trial of low-dose phenelzine in the chronic fatigue syndrome. Infectious Diseases 151, 1150–1153. Psychopharmocology 124, 226–230.
Hudson, M. & Cleare, A. J. (1999). The 1 mg short synacthen test in
Natelson, B. H., Cheu, J., Hill, N., Bergen, M., Korn, L., Denny, T
chronic fatigue syndrome. Clinical Endocrinology 51, 625–630.
& Dahl, K. (1998). Single-blind, placebo phase-in trial of two
escalating doses of selegiline in the chronic fatigue syndrome.
Sharpe, M., Hawton, K., Clements, A. & Cowen, P. (1997). Increased
Neuropsychobiology 37, 150–154.
brain serotonin function in men with chronic fatigue syndrome.
Papadopoulos, E., Crofford, L. J., Engleberg, N. C., Korszun, A.,
British Medical Journal 315, 164–165.
Brucksch, C., Eisner, S. & Demitrack, M. A. (1997). Impaired
Spencer, R. L., Miller, J. T., Moday, H., McEwan, B. S., Blanchard,
HPA axis activity in chronic fatigue syndrome and fibromyalgia.
R. J., Blanchard, D. C. & Sakai, R. R. (1996). Chronic social stress
Presentation at Society of Biological Psychiatry Annual Meeting,
produces reductions in available splenic type II corticosteroid
receptor binding and plasma corticosteroid binding globulin levels.
Peterson, P. K., Pheley, A., Schroeppel, J., Schenck, C., Marshall, P.,
Psychoneuroendocrinology 21, 95–109.
Kind, A., Haugland, M. J., Lambrecht, L. J., Swan, S. &
Stokes, P. E., Stoll, P. M., Koslow, S. H., Maas, J. W., Davis, J. M.,
Goldsmith, S. (1998). A preliminary placebo-controlled crossover
Swann, A. C. & Robins, E. (1984). Pre-treatment DST and
trial of fludrocortisone for chronic fatigue syndrome. Archives of
hypothalamic–pituitary–adrenocortical
Internal Medicine 158, 908–914.
patients and comparison groups. A multicenter study. Archives of
Pincus, S. M., Hartman, M. L., Roelfsema, F., Thorner, M. O. &
General Psychiatry 41, 257–267.
Veldhuis, J. D. (1999). Hormone pulsatility discrimination via
Strickland, P., Morriss, R., Wearden, A. & Deakin, W. (1998). A
comparison of salivary cortisol in chronic fatigue syndrome,
coarse and short time sampling. American Journal of Physiology
community depression and healthy controls. Journal of Affective277, E948–E957. Disorders 47, 191–194.
Poteliakhoff, A. (1981). Adrenocortical activity and some clinical
Sutton, R., Koob, G., Le Maol, M., Rivier, J. & Vale, W. (1982).
findings in chronic fatigue. Journal of Psychosomatic Research 25,
Corticotrophin-releasing factor produces behavioural activation in
rats. Nature 297, 331–333.
Racciatti, D., Sensi, S., De Remigis, P., Barberio, A., Di Sciascio, T.
Swerdlow, N. R., Geyer, M. A., Vale, W. W. & Koob, G. F. (1986).
& Pizzigallo, E. (1998). Neuroendocrine aspects of chronic fatigue
Corticotrophin-releasing factor potentiates acoustic startle in rats :
syndrome. American Journal of Medicine 104 (5A), 1S–3S.
blockade by chlordiazepoxide. Psychopharmocology 88, 147–152.
Raven, P. & Taylor, N. F. (1996). Sex differences in the human
Tattersall, R. (1999). Hypoadrenia, or ‘ a bit of Addison’s disease ’.
metabolism of cortisol. Endocrine Research 22, 751–755. Medical History 43, 450–467.
Riordain, D., Farley, D., Young, W., Grant, C. & van Heerden, J.
Taylor, T., Dluhy, R. & Williams, G. (1983). Beta-endorphin
(1994). Long term outcome of bilateral adrenalectomy in patients
suppresses adrenocorticotrophin and cortisol levels in normal
with Cushing’s syndrome. Surgery 116, 1088–1093.
human subjects. Journal of Clinical Endocrinology and Metabolism
Schlecte, J. A. & Hamilton, D. (1987). The effect of glucocorticoids
57, 592–596.
on corticosteroid binding globulin. Clinical Endocrinology 27,
Terenius, L. & Wahlstrom, A. (1978). Physiological and clinical
relevance or endorphins. In Centrally Acting Peptides (ed. J.
Scott, L. V. & Dinan, T. G. (1998). Urinary free cortisol excretion in
Hughes), pp. 161–178. Baltimore University Park Press : Maryland.
chronic fatigue syndrome, major depression and in healthy
Thompson, L. M., Rubin, R. T. & McCracken, J. T. (1992).
volunteers. Journal of Affective Disorders 47, 49–54.
Neuroendocrine aspects of primary endogenous depression. 12.
Scott, L. V., Medbak, S. & Dinan, T. G. (1998 a). Blunted adreno-
Receiver operating characteristics and kappa analyses of serum
corticotrophin and cortisol responses to corticotrophin-releasing
and urine cortisol measure in patients and matched controls.
hormone stimulation in chronic fatigue syndrome. Acta Psychi-
Psychoneuroendocrinology 17, 507–515. atrica Scandinavica 97, 450–457.
Van Denderen, J., Boersma, J., Zeinstra, P., Hollander, A. & van
Scott, L. V., Medbak, S. & Dinan, T. G. (1998 b). The low dose
Neerbos, B. (1992). Physiological effects of exhaustive physical
adrenocorticotrophin test in chronic fatigue syndrome and in
exercise in primary fibromyalgia syndrome (PFS) : is PFS a
health. Clinical Endocrinology 48, 733–737.
disorder of neuroendocrine reactivity? Scandinavian Journal of
Scott, L. V., Burnett, F., Medbak, S. & Dinan, T. G. (1998 c). Rheumatology 21, 35–37.
Naloxone-mediated activation of the hypothalamic–pituitary–
Vercoulen, J., Swanink, C., Zitman, F., Vreden, S., Hoofs, M.,
adrenal axis in chronic fatigue syndrome. Psychological Medicine
Fennis, J., Galama, J., van der Meer, J. & Bleijenberg, G. (1996). 28, 285–293.
Randomised, double-blind, placebo-controlled study of fluoxetine
Scott, L. V., Teh, J., Reznek, R., Martin, A., Sohaib, A. & Dinan,
in chronic fatigue syndrome. Lancet 347, 858–861.
Wessely, S., Hotopf, M. & Sharpe, M. (1998). Chronic Fatigue and
T. G. (1999 a). Small adrenal glands in chronic fatigue syndrome :
Chronic Fatigue Syndromes. Oxford University Press : Oxford.
a preliminary computer tomography study. Psychoneuroendo-
Wessely, S., Nimnuan, C. & Sharpe, M. (1999). Functional somatic
crinology 24, 759–768.
syndromes : one or many? Lancet 354, 936–939.
Scott, L. V., Medbak, S. & Dinan, T. G. (1999 b). Desmopressin
White, P. D., Thomas, J. M., Amess, J., Crawford, D. H., Grover,
augments pituitary–adrenal responsivity to corticotropin-releasing
S. A., Kangro, H. O. & Clare, A. W. (1998). Incidence, risk and
hormone in subjects with chronic fatigue syndrome and in healthy
prognosis of acute and chronic fatigue syndromes and psychiatric
volunteers. Biological Psychiatry 45, 1447–1454.
disorders after glandular fever. British Journal of Psychiatry 173,
Sharpe, M. C., Archard, L. C., Banatvala, J. E., Borysiewicz, L. K.,
Clare, A. W., David, A., Edwards, R. H. T., Hawton, K. E. H.,
Wood, B., Wessely, S., Papadopoulos, A., Poon, L. & Checkley, S.
Lambert, H. P., Lane, R. J. M., McDonald, E. M., Mowbray,
(1998). Salivary cortisol profiles in chronic fatigue syndrome.
J. F., Pearson, D. J., Peto, T. E. A., Preedy, V. R., Smith, A. P.,
Neuropsychobiology 37, 1–4.
Smith, D. G., Taylor, D. J., Tyrell, D. A. J., Wessely, S., White, P.,
Yatham, L. N., Morehouse, R. L., Chisholm, B. T., Haase, D. A.,
Behan, P. O., Rose, F. C., Peteres, T. J., Wallace, P. G., Warrell,
MacDonald, D. D. & Marrie, T. J. (1995). Neuroendocrine
D. A. & Wright, D. J. M. (1991). Chronic fatigue syndrome :
assessment of serotonin (5-HT) function in chronic fatigue
guidelines for research. Journal of the Royal Society of Medicine
syndrome. Canadian Journal of Psychiatry 40, 93–95. 84, 118–121.
Young, A., Sharpe, M., Clements, A., Dowling, B., Hawton, K. &
Sharpe, M., Clements, A., Hawton, K., Young, A., Sargent, P. &
Cowen, P. (1996). Increased prolactin response to buspirone in
pituitary–adrenal axis in patients with the chronic fatigue syndrome
chronic fatigue syndrome. Journal of Affective Disorders 41, 71–76.
(neurasthenia). Biological Psychiatry 43, 236–237.
TRAVEL INFO & USEFUL TIPS VISA REQUIREMENTS Visa applications may be obtained at Ethiopia's diplomatic missions overseas. Ethiopian embassies may charge a fee for visas, and usually require an onward air ticket, a yellow-fever vaccination certificate and proof of sufficient funds. HEALTH REQUIREMENTS Prior to entry, visitors should be in possession of a valid
EQUITY OPTIONS Information Circular #04-0772 Derivative Securities December 22, 2004 Members, Member Organizations and Registered Option Principals Ann B. Pierre, Options Research Manager Subject Leucadia National Corporation (LUK) - 3-for-2 Stock Split Adjustment - Revise Adjusted Leap Symbols Leucadia National Corporation (LUK) has declared a 3 -for-2 split of i
 adrenal axis (HPA). Interest led from observa-
tions that conditions of low circulating cortisol
are characterized by debilitating fatigue, forexample in Addison’s disease, and following
bilateral adrenalectomy (Riordain et al. 1994).
adrenal axis (HPA). Interest led from observa-
tions that conditions of low circulating cortisol
are characterized by debilitating fatigue, forexample in Addison’s disease, and following
bilateral adrenalectomy (Riordain et al. 1994).