New Leaf Acupuncture Clinic - New Patient Questionnaire The following information is helpful to the diagnostic procedure and enables us to provide you with better treatment. Name ____________________________ ! Female ! Male Birth Date ___________ Today’s Date __________ Address_____________________________________________________________________________________________ E-mail address ____________________________________________________Phone_____________________________ Marital Status __________________ No. of Children ________ Occupation_____________________________________ Emergency Contact Name _______________________________________ Phone _______________________________ Doctor_______________________________________________________________________________________________ Is this your first time getting acupuncture? !Yes ! No. How did you hear about us?________________________ Goals: What would you most like to achieve with acupuncture treatments? _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ Major Symptoms: Please list in order of importance what symptoms are of concern to you. (most concerning to least, along with the duration of the symptom) _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ _____________________________________________________________________________________________________
Experiencing pain/discomfort in any area of your body? !Yes !No
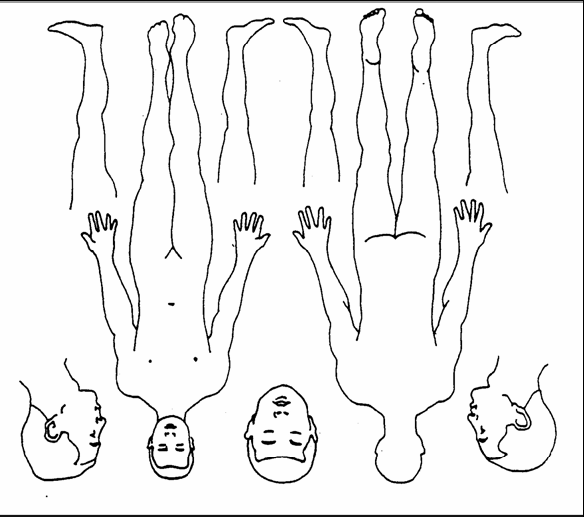
Please rate your pain level: < 1 2 3 4 5 6 7 8 9 10 > Duration of pain: ____________ Use the illustration to indicate painful or distressed areas. Indicate the location of the discomfort by using the symbol that best describes the feeling: X X XSharp/StabbingP P PPins & Needles D D DDull/AchingN N NNumbness T T TTightness/Spasms
Aggravating factors: (eg. Heat) ____________________Alleviating factors: (eg. Cold) ______________________
Medical History Do you or have you had any of the following conditions? If yes, please indicate date of diagnosis. Date Diagnosed Date Diagnosed
Cancer (type) ____________________________________
Hepatitis _____________________________________
HIV _____________________________________________
Stroke _______________________________________
Diabetes ________________________________________
High Blood Pressure __________________________
Mental Illness ____________________________________
Thyroid Disease ______________________________
Heart Disease ____________________________________
High Cholesterol ______________________________
Seizures _________________________________________
Other ________________________________________
Please list any surgeries or major injuries with dates. _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ List any medications or supplements you have taken in the last 2 months. _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ Do you have a pacemaker or any metal devices in your body? !Yes ! No. If so, which: ____________________ Intolerant of, or allergic to: ! Alcohol Swabs ! Iodine ! Arnica Cream ! Bio Oil Family History Indicate close family members with any of the following: Family member(s) Family Member(s)
Cancer (specify type) _____________________________
Heart Disease ________________________________
High Cholesterol _________________________________
Stroke _______________________________________
Diabetes ________________________________________
High Blood Pressure __________________________
Mental Illness ___________________________________
Alcoholism ___________________________________
Lifestyle Habits
Do you have an exercise routine? !Yes ! No Please describe ______________________________________________________________________________________ _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ How many hours per night do you sleep on average? __________ Do you wake rested? !Yes ! No Nicotine Use: __________________ Alcohol Use (#drinks/week and type):____________________________________ Caffeine Use (#drinks/day and type): ____________________Water intake (how much/day): ____________________ Briefly describe your dietary habits (#meals/day; type of food; snacks; sweet tooth) _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ Energy: How is your energy?
Please circle. Low < 1 2 3 4 5 6 7 8 9 10 > High
What time of day is your energy: Highest: !6am-12pm !1pm-5pm !6pm-12am Lowest: !6am-12pm !1pm-5pm !6pm-12am Do you fatigue easily? !Yes ! No How do you feel emotionally? _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ Emotions: How are your stress levels?
Please circle. Low < 1 2 3 4 5 6 7 8 9 10 > High
Do you have: ! Panicattacks ! Depression ! Anxiety/Worry ! Irritability ! Nervousness ! Fear attacks ! Mood Swings ! Difficulty Making Decisions ! Poor memory ! Difficult concentration ! Suppressing Emotions ! Frequent Sighing ! Easily Startled Bowel movements: Urination:
How often?___time(s) a day, or __ time(s) a week
Please tick symptoms you have or have had in the past year: Respiratory/Cardiovascular Energy and Immunity
!Heart Palpitations / Fluttering
!Poor Circulation (Cold hands/feet)
Male Health
!Particularly sensitive to the cold
Head, Eye, Ear, Nose, and Throat Musculoskeletal Gastrointestinal
!Finger Pain / Tingling / Numbness
Neurological Kidney/Urinary
!Frequent Urinary Tract Infections
!Dry / Itchy Skin !Brittle Nails
Women Only:
Currently Pregnant? !Yes ! No
!Vaginal discharge. Colour?_____
Female Health
. . . !before !during !after
Acupuncture Appointments
Please bring this completed new patient questionnaire with you to your first appointment. Please bring or wear loose clothing (shorts, t-shirts) to each appointment. Please eat a light meal or snack before your appointment; an empty stomach may cause dizziness. Please do not eat or drink food that may change the color of your tongue or brush your tongue the day of your appointment. (coffee, fizzy drinks, juice, liquorice, beetroot, etc) While contra-indications for acupuncture are rare and, although also rare, sometimes a small local bruise can occur. What to expect at your first visit?
Your first visit will take a little over one hour and will include an acupuncture treatment. We will discuss your health questionnaire and any concerns you have prior to the treatment. I will make a diagnosis, a treatment plan and may give a few suggestions regarding your condition. If you have any questions please do not hesitate to email or call me at: niall@newleaf.ie (087) 2632732 Niall O’Leary New Leaf Acupuncture Clinics: 212 Kimmage Road Lower, Dublin 6w 50 Marian Road, Rathfarnham, Dublin 14 15 Grantham St, Portobello, Dublin 8 Financial Policy, etc
Payment is due at time of service for all patients. A fee will be charged for missed appointments or cancellations without a 24-hour notification. I also understand that these treatments may produce some bruising and I release the practitioner from liability in the event that that should occur. ________________________________________ ____________________ Signature
________________________________________ Please Print Name
This is a summary of benefits for your Pharmacy Plan. The document will be used to reflect how your Pharmacy plan will be loaded (Pharmacy plan deductibles, out-of-pocket maximums, copays and annual maximums do not integrate with the employer medical program unless elected as part of the CIGNA Choice Fund product) CIGNA Healthcare Pharmacy Customer Worksheet Tektronix, Inc. CIGNA
30 Seconds to Save a LifeABIGAIL HALPERIN MD, MPH, DEPT OF FAMILY MEDICINE, UNIVERSITY OF WASHINGTON, SEATTLETIM MCAFEE MD, MPH, CHIEF MEDICAL OFFICER, FREE & CLEAR, INC., SEATTLEOne of the greatest joys for us, as family physicians,with their care than those who are not. Further, referralis to help patients make behavior changes that will allowto a convenient, evidence-based treatment p
 New Leaf Acupuncture Clinic - New Patient Questionnaire
New Leaf Acupuncture Clinic - New Patient Questionnaire