Modifying clopidogrel maintenance doses according to vasodilatorstimulated phosphoprotein phosphorylation index improves clinical outcome in patients with clopidogrel resistance
Address for correspondence: Yan Lai, MM Clinical Investigation
Department of CardiologyShanghai East HospitalTongji University School of Medicine
Phosphoprotein Phosphorylation IndexImproves Clinical Outcome in PatientsWith Clopidogrel Resistance
Xiao-dong Wang, MD; Dai-fu Zhang, MM; Shao-wei Zhuang, MD; Yan Lai, MM
Department of Cardiology, Shanghai East Hospital, Tongji University School of Medicine,
Background: Despite dual antiplatelet therapy, the rate of major adverse cardiovascular events (MACE) afterpercutaneous coronary intervention (PCI) remains high. Ex vivo tests of clopidogrel resistance can predict
MACE after PCI. The purpose of this study is to evaluate the clinical impact of adjusting phosphorylationanalysis in patients with clopidogrel resistance undergoing PCI. Hypothesis: We hypothesized that VASP-guided clopidogrel maintenance doses, compared to fixed doses,improved clinical outcome. Methods: This monocentric, prospective, randomized study was performed on 306 patients undergoingPCI. Patients were randomized to a control group (n = 156) and to a vasodilator-stimulated phosphoprotein(VASP)-guided group (n = 150). In the VASP-guided group, patients received adjusted maintenance doses ofclopidogrel to obtain platelet reactivity index (PRI) of <50% during 1 year after PCI. The primary endpoint wasthe rate of MACE. The secondary endpoints were major and minor bleeding. Results: All patients completed the PCI procedure and 298 patients completed follow-up. The control andVASP-guided groups had similar demographic, clinical, and angiographic characteristics. In the VASP-guided
group, PRI was significantly decreased (from 72.1% ± 11.4% to 27.7% ± 8.4%; P = 0.001) in 128 patients(87.1% of all participants). During the 1-year follow-up, 14 MACEs were recorded in the VASP-guided group
and 30 MACEs were recorded in the control group (9.3% vs 20.4%, respectively; P = 0.008). There was nodifference in the rate of major and minor bleeding in the VASP-guided group compared with the control group(12.9% vs 16.6%; P = 0.06). Conclusions: Modifying clopidogrel maintenance doses according to platelet reactivity monitoring decreasesthe rate of MACE after PCI without increasing bleeding in patients with clopidogrel resistance during 1-year
Introduction
implemented, recurrent thrombotic events and in-stent
During the last decade, angioplasty has become the most
thrombosis still occur, which are associated with significant
popular method of coronary revascularization. Since the
mortality and morbidity.6–9 These clinical findings have
mid-1990s, stent implantation has been the dominant
put forward concern about antiplatelet-therapy resistance.
procedure to reduce the rate of acute occlusion1 and in-
Aspirin resistance is recognized, and several strategies are
stent restenosis.2,3 In addition, dual antiplatelet therapy
recommended.10 More recently, the concept of biological
with aspirin and clopidogrel has greatly decreased the
resistance to clopidogrel has caused much attention.
risk of major adverse cardiovascular events (MACE)
Interindividual variability in platelet response to clopidogrel
after percutaneous coronary intervention (PCI).4,5 Although
is known to be large. Poor responders represent between
the addition of thienopyridines to aspirin is widely
10% and 40% of patients receiving therapy, depending on thetests and thresholds used.11–13
Several methods have been developed to deal with
This project was sponsored by Science and Technology
clopidogrel resistance,14 of which the most popular strategy
Commission of Shanghai Municipality (No. SK08-6). The
is increasing the loading dose (LD) utilized in patients
authors have no other funding, financial relationships, or
undergoing PCI to 600 mg15–18 and 900 mg.19,20 Although
clopidogrel response is dose-dependent, there is a threshold
Clin. Cardiol. (in press) 1
Published online in Wiley Online Library (wileyonlinelibrary.com)
DOI:10.1002/clc.20884 2011 Wiley Periodicals, Inc.
to its platelet-inhibitory effect when certain doses are
heparin was initiated in the intensive care unit before PCI.
administrated.19,20 In order to find a better method to
Glycoprotein IIb/IIIa inhibitors were not used.
tackle clopidogrel resistance, Bonello et al21 adjusted theclopidogrel LD according to platelet monitoring using the
Clopidogrel Modification
vasodilator-stimulated phosphoprotein (VASP) index in a
One month after PCI, clopidogrel administration was
multicenter randomized prospective study, and observed
adjusted according to VASP index to keep PRI <50%. The
that it was safe and significantly improved the clinical
timing of VASP monitoring was 3, 6, 9, and 12 months after
outcomes after PCI in patients with clopidogrel resistance.
first PRI analysis. Clopidogrel doses were increased in a
In another study, Bonello et al22 also demonstrated that
stepwise manner: After the first PRI monitoring (1 month
tailoring the clopidogrel LD according to platelet reactivity
after PCI), 150 mg clopidogrel was administered if PRI was
monitoring decreased the rate of early stent thrombosis
>50%. At the second PRI monitoring, 3 months later, a dose
(ST) after PCI without increasing bleeding. These 2
of 225 mg clopidogrel was given to patients if PRI remained
studies prove the significance of VASP-guided antiplatelet
at >50%. Another 75 mg of clopidogrel would be added every
therapy in clopidogrel-resistant patients. However, the
3 months if PRI >50%. At the end of 1 year, the maximum
relationship between a clopidogrel maintenance dose (MD)
MD of clopidogrel would be 375 mg. If PRI was <25% at
and the rate of MACE after initiation of dual antiplatelet
that time point, the clopidogrel dose would be decreased
therapy >1 month is still uncertain. In the present study,
to 75 mg daily. If PRI fluctuated between 25% and 50%, the
we investigate the impact of a tailored clopidogrel MD
determined dose would be maintained.
according to platelet reactivity monitoring on the rate ofMACE in patients after primary PCI during a 1-year period. Blood Samples
Blood samples for PRI analysis were drawn by venipuncture
of the antecubital vein. The initial blood drawn was discarded
Patients
to avoid measuring platelet activation induced by the needle
A monocentric, prospective study was undertaken in the
puncture. Blood was collected into a tube containing 3.8%
cardiology department of the university hospital. The
trisodium citrate. The tube was inverted 3 to 5 times for
study protocol was in accordance with the Declaration of
gentle mixing and sent immediately to the hemostasis
Helsinki and approved by the local ethics committee of
our institution. All patients gave written informed consentbefore inclusion. Patients were enrolled in the study 1 month
VASP Phosphorylation Analysis
after undergoing PCI for one of 3 indications: refractory
The VASP phosphorylation analysis was performed within
angina pectoris in addition to optimal medical therapy, silent
1 hour of blood collection by an experienced investigator
ischemia on thallium scintigraphy, or non–ST-elevation
using a platelet VASP kit (Becton Dickinson, Franklin Lakes,
acute coronary syndrome. Other inclusion criteria were
NJ) according to the manufacturer’s instructions.24 Briefly,
patient age >18 years and <80 years, and platelet reactivity
blood samples were incubated in vitro with adenosine
index (PRI) <50%. The exclusion criteria were a history
diphosphate (ADP) and/or prostaglandin E1 (PGE1) before
of bleeding diathesis, persistent ST-segment elevation
fixation. Each sample was indirectly immunolabeled by
acute coronary syndrome (ACS), elevated levels of cardiac
incubation with 16C2 fluorescein isothiocyanate (FITC)
markers, New York Heart Association functional class III or
followed by staining with a goat antimouse FITC polyclonal
IV, contraindications to antiplatelet therapy, platelet count
reagent (Becton Dickinson, Franklin Lakes, NJ). Flow
<100× 109/L, creatinine clearance <25 mL/minute, use
cytometric analysis was performed using a Coulter EPICS
of a glycoprotein IIb/IIIa inhibitor, sudden death, and
XL cytometer (FACSCalibur, BD, Franklin Lakes, NJ).
concurrent severe illness with expected survival <1 year.
Platelet population was identified on its forward andside scatter distributions, and 3000 platelet events were
Angioplasty Procedure
gated and analyzed for mean fluorescence intensity (MFI)using EPICS XL software. The MFI corresponding to
Percutaneous coronary intervention was carried out
each experimental condition (ADP, ADP + PGE1) was
according to international guidelines, using a standard
determined to establish a ratio directly correlated with
technique, through the radial route.23 A drug-eluting
the VASP phosphorylation state. The ratio, [(MFI
stent could be used according to American College
of Cardiology/American Heart Association (ACC/AHA)
ADP + PGE1)/MFIPGE1] × 100, is expressed in this
study as a platelet reactivity index (PRI) corresponding to a
guidelines. An intravenous bolus of unfractionated heparin
ratio of the VASP phosphorylation of activated platelets vs
(100 IU/kg) was administered at the beginning of the
resting platelets and is expressed as a percentage of platelet
procedure. The sheath was removed immediately at
reactivity. The intra-assay coefficient of variation was <5%
the end of the procedure in all cases. Combination
and the interassay coefficient of variation was <8%.
usage of 100 mg aspirin and 300 mg clopidogrel LD wasadministered before PCI. After PCI, the combinationadministration of 100 mg aspirin and clopidogrel was
The Early PCI Procedural Outcome
continued and the MD of clopidogrel fluctuated between 75
Stent thrombosis was classified as subacute when it
and 375 mg for ≥ 1 year. For patients with non–ST-segment
occurred from the end of the PCI procedure up to 30 days
elevation ACS, anticoagulation with low-molecular-weight
later and was classified as late when it occurred after
2 Clin. Cardiol. (in press)
X. Wang et al: VASP-guided clopidogrel maintenance dosesPublished online in Wiley Online Library (wileyonlinelibrary.com)DOI:10.1002/clc.20884 2011 Wiley Periodicals, Inc.
30 days. Subacute and late ST were defined according to
Baseline characteristics are summarized in Table 1.
Demographic data and clinical characteristics were similarin the 2 groups. The prevalence of cardiovascular riskfactors was similar, including diabetes and current smoking
Clinical Endpoints
(P = 0.5 and P = 0.6, respectively). The PCI indications
Clinical follow-up was initiated 1 month after PCI. Endpoints
were balanced among the 3 inclusion criteria and were
were recorded by an investigator who was not aware of the
similar between the 2 randomized groups. The rates of
treatment status and clinical characteristics of patients. The
patients undergoing PCI for non–ST-elevation ACS were
primary endpoint was the rate of MACE, which included
similar (20% vs 20%, P = 0.7). The 2 groups did not differ
cardiovascular death, angiographically confirmed ST,
in left ventricular ejection fraction (P = 0.6). The PCI
recurrent ACS defined by the ACC/AHA guidelines,23 and
data was also similar including the number and length
recurrent revascularization by either coronary angioplasty
of drug-eluting stents per patient (P = 0.4 and P = 0.2,
or bypass surgery. Secondary endpoints, recorded to assess
safety, were major and minor bleeding. Major bleedingwas defined as intracranial bleeding or clinically overtbleeding associated with a decrease in hemoglobin of
Platelet Reactivity Index
50 g/L, according to the Thrombolysis in Myocardial
We analyzed post-treatment platelet function using the flow
Infarction (TIMI) criteria.26 Minor bleeding was also defined
cytometric assessment of VASP phosphorylation at a mean
according to TIMI criteria.26 Drug-therapy compliance was
time of 1, 3, 6, 9, and 12 months after the patients were
randomized to the 2 groups (Table 2). The baseline PRI
The treating physician and the investigators who
after PCI showed no significant difference between the
evaluated the clinical endpoints were blind to the results
2 groups (69.3% ± 18% for the control group vs 72.1%
of platelet testing and to group assignment. Prespecified
± 11.4% for the VASP-guided group, P = 0.4). In the
clinical and laboratory data during hospitalization periods
follow-up at 12 months, PRI in the VASP-guided group had
were obtained from hospital charts reviewed by independent
decreased significantly from the baseline (27.7% ± 8.4%
research personnel who were unaware of the objectives of
vs 72.1% ± 11.4%, P = 0.001). The 12-month PRI in the
the study. Clinical follow-up was conducted by telephone
control group also declined, but did not change significantly
contact or office visits. All clinical events were adjudicated
(66.4% ± 18.6% vs 69.3% ± 18%, P > 0.05). The intervening
by independent physicians unaware of treatment status of
PCIs for the 3-month, 6-month, and 9-month follow-ups are
the patients and not involved in the study.
also included in Table 2. Compared with the control group,the PRI in the VASP-guided group decreased significantlyat each follow-up period (P = 0.03, P < 0.001, P = 0.04,
Statistical Analysis
Statistical analysis was performed using SPSS version 16.0
In the VASP-guided group, the numbers of patients
software (SPSS Inc., Chicago, IL). Continuous variables
receiving clopidogrel dose modification were 101 (66.9%,
are expressed as mean ± SD. Categorical variablesare expressed as frequency and percentage. Comparisonbetween categorical variables was performed using the
χ2 test or Fisher exact test when frequencies were <5.
Analysis of variance was used to compare characteristicsof quantitative variables. Kaplan-Meier curves were used to
assess MACE-free survival. Differences between the curves
were tested with a log-rank statistic. Patients’ Demographic, Biological, and Angiographic Characteristics
From August 2008 to October 2009, 538 continuous patientsadmitted to the university hospital cardiology center wereprospectively screened for inclusion (Figure 1). In total, 232patients were not included: 20 met the exclusion criteria,
and 212 had a PRI <50% after 1 month MD of clopidogrel;
therefore, they were considered good responders and werenot included in the study. A total of 306 patients had a PRI>50% and were included and randomized to the controlgroup (n = 156) or the VASP-guided group (n =1 50). Five
patients in the control group and 3 patients in the VASP-guided group were lost to follow-up. Ultimately, 151 patientsin the control group and 147 patients in the VASP-guided
Figure 1. Study design and flow chart. Abbreviations: VASP,
vasodilator-stimulated phosphoprotein.
Clin. Cardiol. (in press) 3
X. Wang et al: VASP-guided clopidogrel maintenance doses
Published online in Wiley Online Library (wileyonlinelibrary.com)
DOI:10.1002/clc.20884 2011 Wiley Periodicals, Inc.
Abbreviations: ACE, angiotensin-converting enzyme; BMI, body massindex; Ca, calcium; CABG, coronary artery bypass grafting; CAD,
coronary artery disease; Cr, creatinine; DM, diabetes mellitus; HT,hypertension; LVEF, left ventricular ejection fraction; MD, maintenance
dose; MI, myocardial infarction; NST ACS, non–ST-elevation acute
coronary syndrome; PCI, percutaneous coronary intervention; VASP,vasodilator-stimulated phosphoprotein. The Early PCI Procedural Outcome
The rate of early ST was not significantly different betweenthe control group and the VASP-guided group (4.7% vs 3.9%,
P = 0.3; Table 3). All ST were recorded within 30 days after
PCI. There were 2 cases of acute ST (0.9%) and 6 of subacuteST (3.7%) in the control group. In the VASP-guided group,
the rate of acute ST was 0.8% and the rate of subacute ST was3.2%. During 1 month after PCI, 7 patients (2.3%) underwent
PCI again because of recurrent myocardial infarction, 3 in
the control group and 4 in the VASP-guided group. Primary Endpoints During Follow-Up
In the follow-up at 12 months, 3 patients in the VASP-guided group and 5 patients in the control group were
lost to follow-up. The loss rate was 7.5%. During follow-up, 30 (19.2%) MACE in the control group and 14 (9.3%)
MACE in the VASP-guided group occurred, resulting in a
statistically difference between the 2 groups (P = 0.008). The distribution of cardiovascular events is summarized in
Kaplan-Meier Analysis
Cumulative survival in the 2 groups (Figure 2) was
distinguished by the Kaplan-Meier curve. In the first
6 months, survival was significantly different. But after that,
the difference stabilized and did not increase. Fewer patientsdied in the VASP-guided group. Secondary Endpoints and Side Effects of Clopidogrel
There were no major hemorrhagic complications in either
group (Table 4). Both the major and minor bleeding events
between the 2 groups were not significantly different. Discussion The present study suggests that modifying clopidogrel MDs
3 months), 119 (78.8%, 6 months), 121 (80.1%, 9 months),
according to VASP index improves the clinical outcome in
and 131 (87.1%, 12 months), respectively. At the end of the
clopidogrel-resistant patients undergoing PCI. This strategy
study, 20 of 151 patients (13.9%) in the VASP-guided group
of clopidogrel MD adjustment is safe and is not associated
still had the high PRI profile, at >50%. 4 Clin. Cardiol. (in press)
X. Wang et al: VASP-guided clopidogrel maintenance dosesPublished online in Wiley Online Library (wileyonlinelibrary.com)DOI:10.1002/clc.20884 2011 Wiley Periodicals, Inc.
Table 2. PRI in the 2 Groups During 1-Year Follow-Up
Abbreviations: PRI, platelet reactivity index; VASP, vasodilator-stimulated phosphoprotein.
Table 3. Early Definite ST During 1-Month Follow-Up After Primary PCI
Abbreviations: DST, definite stent thrombosis; PCI, percutaneouscoronary intervention; ST, stent thrombosis; VASP, vasodilator-stimulated phosphoprotein.
The rates of diabetes mellitus and current smoking are
higher in the control group, but the difference is notsignificant. These 2 demographic characteristics do not
Figure 2. Kaplan-Meier analysis for 1-year follow-up. Log-rank P < 0.01.
Group 1 refers to the control group; group 2 refers to the VASP-guided
In cases of clopidogrel resistance, authors have recom-
group; time is given in days. Abbreviations: Cum, cumulative.
mended new antiplatelet agents ticlopidine, prasugrel,27ticagrelor,28
clopidogrel15–20 is also recommended. However, ticlopidine
substrate of both cAMP-dependent and cGMP-dependent
increases risk of bleeding27–29 or dyspnea.30 In addition,
protein kinases. Analysis of the VASP phosphorylation ratio
increasing LDs of clopidogrel does not confer more clini-
can be used for measuring various signal transduction pro-
cal benefit.19,20 In recent years, several studies have been
cesses, including dephosphorylation following P2Y12 ADP
launched focusing on VASP-guided clopidogrel modification
receptor activation and its reversal by P2Y12 antagonists.31,32
in patients on clopidogrel. Vasodilator-stimulated phospho-
In vitro tests of VASP phosphorylation analysis accurately
protein is an intracellular actin-regulatory protein that is a
detect biological clopidogrel resistance that is associatedwith worse outcome after PCI.33–35 Bonello et al21 demon-strated that PRI using VASP monitoring is safe and sig-
Table 4. Major and Minor Clinical Endpoints During 1-Year Follow-Up
nificantly improves clinical outcome after a 600-mg LD.
Furthermore, a tailored 600-mg clopidogrel LD according
to PRI also prevents acute and subacute ST in the samepatients.22 However, these 2 studies were conducted within
1 month after stent implantation. In the present study, we
report that the benefit of VASP-guided clopidogrel therapy
lasts for 12 months. It confirms that VASP-guided clopido-grel dose modification relieves clopidogrel resistance and
In a retrospective study, Barragan et al33 observed
a strong correlation between subacute ST and a PRI
>50%. The result was later confirmed in a prospective
study, and the 50% threshold demonstrated a very highnegative predictive value for MACE after PCI.36 In a recent
experimental study, Schumacher et al37 demonstrated thata 50% PRI corresponded to a nearly 90% P2Y
blockage. So we used 50% PRI as the cutoff point.
Abbreviations: ACS, acute coronary syndrome; MACE, major adverse
Our study shows that the MACE occurred during the first
cardiac events; ST, stent thrombosis.
6 months in the follow-up period. In the latter 6 months of
Clin. Cardiol. (in press) 5
X. Wang et al: VASP-guided clopidogrel maintenance doses
Published online in Wiley Online Library (wileyonlinelibrary.com)
DOI:10.1002/clc.20884 2011 Wiley Periodicals, Inc.
follow-up, the difference in the incidence of MACE between
Gurbel PA, Bliden KP, Hiatt BL, et al. Clopidogrel for coronary
the 2 groups remained stable. The results indicate that the
stenting response variability, drug resistance, and the effect ofpretreatment platelet reactivity. Circulation. 2003;107:2908–2913.
effect of clopidogrel in preventing thrombosis occurs pri-
Angiolillo DJ, Fern`andez-Ortiz A, Bernardo E. Variability in indi-
marily within 6 months, which is in accordance with Airoldi’s
vidual responsiveness to clopidogrel clinical implications, man-
findings in a prospective observational cohort study.38
agement, and future perspectives. J Am Coll Cardiol. 2007;49:
We observed no increase in bleeding in the VASP-guided
group, despite the use of the clopidogrel MD. This may be
Angiolillo DJ, Fern`andez-Ortiz A, Bernardo E, et al. High clopi-dogrel loading dose during coronary stenting: effects on drug
because platelet monitoring stratifies the dose of clopidogrel
response and interindividual variability. Eur Heart J. 2004;25:
according to the individual response, preventing high-dose
usage in patients with good response.
Gurbel PA, Bliden KP, Hayes KM, et al. The relation of dosingto clopidogrel responsiveness and the incidence of high post-treatment platelet aggregation in patients undergoing coronary
Conclusion
stenting. J Am Coll Cardiol. 2005;45:1392–1396.
Hochholzer W, Trenk D, Frundi D, et al. Time dependence of
This monocentric, prospective, randomized study demon-
platelet inhibition after a 600-mg loading dose of clopidogrel in
strates that tailoring clopidogrel MD according to platelet
a large, unselected cohort of candidates for percutaneous coronary
reactivity measured by PRI is safe and may significantly
intervention. Circulation. 2005;111:2560–2564.
improve clinical outcome after PCI in patients with clopido-
Patti G, Colonna G, Pasceri V, et al. Randomized trial of highloading dose of clopidogrel for reduction of periprocedural
myocardial infarction in patients undergoing coronary intervention:results from the ARMYDA-2 (Antiplatelet Therapy for Reductionof Myocardial Damage during Angioplasty) study. Circulation.Acknowledgments
The authors extend sincere thanks to the patients for their
Von Beckerath N, Taubert D, Pogatsa-Murray G, et al. Absorption,
willingness to participate in the study. We also thank Ying
metabolization, and antiplatelet effects of 300-, 600-, and 900-mg loading doses of clopidogrel: results of the ISAR-CHOICE
(Intracoronary Stenting and Antithrombotic Regimen: ChooseBetween 3 High Oral Doses for Immediate Clopidogrel Effect)Trial. Circulation. 2005;112:2946–2950. References
Montalescot G, Sideris G, Meuleman C, et al. A randomized
Sigwart U, Urban P, Golf S, et al. Emergency stenting for acute
comparison of high clopidogrel loading doses in patients with
occlusion after coronary balloon angioplasty. Circulation. 1988;
non-ST-elevation acute coronary syndromes: the ALBION trial. J Am Coll Cardiol. 2006;48:931–938.
Serruys PW, de Jaegere P, Kiemeneij F, et al. A comparison of
Bonello L, Camoin-Jau L, Arques S, et al. Adjusted clopidogrel
balloon-expandable-stent implantation with balloon angioplasty in
loading doses according to vasodilator-stimulated phosphoprotein
patients with coronary artery disease. Benestent Study Group.
phosphorylation index decrease rate of major adverse cardiovascu-
N Engl J Med. 1994;331:489–495.
lar events in patients with clopidogrel resistance. J Am Coll Cardiol.
Fischman DL, Leon MB, Baim DS, et al. A randomized comparison
of coronary-stent placement and balloon angioplasty in the treat-
Bonello L, Camoin-Jau L, Armero S, et al. Tailored clopidogrel
ment of coronary artery disease. N Engl J Med. 1994;331:496–501.
loading dose according to platelet reactivity monitoring to prevent
Bertrand ME, Rupprecht HJ, Urban P, et al. Double-blind study
acute and subacute stent thrombosis. Am J Cardiol. 2009;103:5–10.
of the safety of clopidogrel with and without a loading dose in
Kushner FG, Hand M, Smith SC Jr, et al. 2009 Focused Updates:
combination with aspirin compared with ticlopidine in combination
ACC/AHA Guidelines for the Management of Patients With ST-
with aspirin after coronary stenting: the Clopidogrel Aspirin
Elevation Myocardial Infarction (Updating the 2004 Guideline
Stent International Cooperative Study (CLASSICS). Circulation.
and 2007 Focused Update) and ACC/AHA/SCAI Guidelines on
Percutaneous Coronary Intervention (Updating the 2005 Guideline
Mehta SR, Yusuf S, Peters RJ, et al. Effects of pretreatment with
and 2007 Focused Update). J Am Coll Cardiol. 2009;54:2205–2241.
clopidogrel and aspirin followed by long-term therapy in patients
Bonello L, Paganelli F, Arpin-Bornet M, et al. Vasodilator-
undergoing percutaneous coronary intervention: the PCI-CURE
stimulated phosphoprotein phosphorylation analysis prior to per-
study. Lancet. 2001;358:527–533.
cutaneous coronary intervention for exclusion of postprocedu-
Serruys PW, Strauss BH, Beatt KJ, et al. Angiographic follow-up
ral major adverse cardiovascular events. J Thromb Haemost.
after placement of a self-expanding coronary-artery stent. N Engl J
Cutlip DE, Windecker S, Mehran R, et al; Academic Research
Schatz RA, Baim DS, Leon M, et al. Clinical experience with the
Consortium. Clinical end points in coronary stent trials: a case
Palmaz-Schatz coronary stent. Initial results of a multicenter study.
for standardized definitions. Circulation. 2007;115:2344–2351. Circulation. 1991;83:148–161.
Rao AK, Pratt C, Berke A, et al. Thrombolysis in Myocardial
omig A, Neumann FJ, Kastrati A, et al. A randomized compar-
Infarction (TIMI) Trial—phase I: hemorrhagic manifestations
ison of antiplatelet and anticoagulant therapy after the placement
and changes in plasma fibrinogen and the fibrinolytic system
of coronary-artery stents. N Engl J Med. 1996;334:1084–1089.
in patients treated with recombinant tissue plasminogen activator
Haude M, Erbel R, Issa H, et al. Subacute thrombotic complica-
and streptokinase. J Am Coll Cardiol. 1988;11:1–11.
tions after intracoronary implantation of Palmaz-Schatz stents. Am
Wiviott SD, Braunwald E, McCabe CH, et al. Prasugrel versus
clopidogrel in patients with acute coronary syndromes. N Engl
Tantry US, Mahla E, Gurbel PA. Aspirin resistance. Prog Cardio-
Wallentin L, Becker RC, Budaj A, et al. Ticagrelor versus clopido-
Aleil B, Ravanat C, Cazenave JP, et al. Flow cytometric analysis of
grel in patients with acute coronary syndromes. N Engl J Med.
intraplatelet VASP phosphorylation for the detection of clopidogrel
resistance in patients with ischemic cardiovascular diseases.
Harrington RA, Stone GW, McNulty S, et al. Platelet inhibition
J Thromb Haemost. 2005;3:85–92.
with cangrelor in patients undergoing PCI. N Engl J Med.
Lepantalo A, Virtanen KS, Heikkila J, et al. Limited early anti-
platelet effect of 300 mg clopidogrel in patients with aspirin therapy
Storey RF, Bliden KP, Patil SB, et al. Incidence of dyspnea and
undergoing percutaneous coronary interventions. Eur Heart J.
assessment of cardiac and pulmonary function in patients with
stable coronary artery disease receiving ticagrelor, clopidogrel,
6 Clin. Cardiol. (in press)
X. Wang et al: VASP-guided clopidogrel maintenance dosesPublished online in Wiley Online Library (wileyonlinelibrary.com)DOI:10.1002/clc.20884 2011 Wiley Periodicals, Inc.
or placebo in the ONSET/OFFSET study. J Am Coll Cardiol.
Cuisset T, Frere C, Quilici J, et al. High post-treatment platelet
reactivity identified low-responders to dual antiplatelet therapy at
increased risk of recurrent cardiovascular events after stenting
focal adhesion vasodilator-stimulated phosphoprotein at Ser157
for acute coronary syndrome. J Thromb Haemost. 2006;4:
in intact human platelets correlates with fibrinogen receptor
inhibition. Eur J Biochem. 1994;225:21–27.
Cuisset T, Frere C, Quilici J, et al. Benefit of a 600-mg loading
Schwarz UR, Geiger J, Walter U, et al. Flow cytometric analysis of
dose of clopidogrel on platelet reactivity and clinical outcomes
intracellular VASP phosphorylation for the assessment of activating
in patients with non-ST-segment elevation acute coronary
and inhibitory signal transduction pathways in human platelets.
syndrome undergoing coronary stenting. J Am Coll Cardiol.J Thromb Haemost. 1999;82:1145–1152.
Barragan P, Bouvier JL, Roquebert PO, et al. Resistance to
Schumacher WA, Bostwick JS, Ogletree ML, et al. Biomarker
thienopyridines: clinical detection of coronary stent thrombosis
optimization to track the antithrombotic and hemostatic effects
by monitoring of vasodilator-stimulated phosphoprotein phospho-
of clopidogrel in rats. J Pharmacol Exp Ther. 2007;322:369–377.
rylation. Catheter Cardiovasc Interv. 2003;59:295–302.
Airoldi F, Colombo A, Morici N, et al. Incidence and predictors of
Matetzky S, Shenkman B, Guetta V, et al. Clopidogrel resistance
drug-eluting stent thrombosis during and after discontinuation of
is associated with increased risk of recurrent atherothrombotic
thienopyridine treatment. Circulation. 2007;116:745–754.
events in patients with acute myocardial infarction. Circulation. 2004;109:3171–3175.
Clin. Cardiol. (in press) 7
X. Wang et al: VASP-guided clopidogrel maintenance doses
Published online in Wiley Online Library (wileyonlinelibrary.com)
DOI:10.1002/clc.20884 2011 Wiley Periodicals, Inc.
In vitro Performance Characterization of the New Sidestream® Plus Breath-Enhanced Jet Nebulizer J.P. Young, T.J. Hurren, R.K. Harrington, R.H.M. Hatley, T. Dyche Respironics Respiratory Drug Delivery (UK) Ltd, Chichester Business Park, Chichester, West We compared in vitro the performance of a new breath-enhanced Sidestream Plus ® (SP) nebulizer (NEB) in t
f : {0, 1}32 × {0, 1}48 → {0, 1}32. These notes are based in part on Susan Landau’sYou can find a pictorial representation of f in Fig-paper: “Standing the test of time: the data en-ure 4.5. Here is how f (A, J) is computed:1. Expand A to a bitstring of length 48, using aDES was adopted in 1977 as a standard for “un-2. Compute E(A) ⊕ J. View E(A) ⊕ J as the con-classified” a
 Address for correspondence:
Address for correspondence: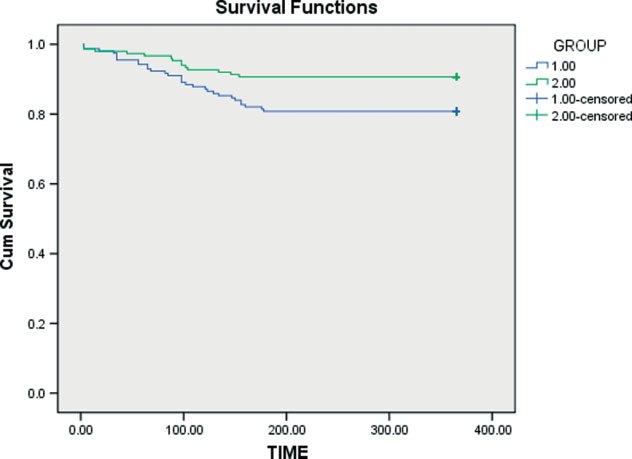 Table 2. PRI in the 2 Groups During 1-Year Follow-Up
Abbreviations: PRI, platelet reactivity index; VASP, vasodilator-stimulated phosphoprotein.
Table 2. PRI in the 2 Groups During 1-Year Follow-Up
Abbreviations: PRI, platelet reactivity index; VASP, vasodilator-stimulated phosphoprotein.