International Journal of Medical Informatics 51 (1998) 59 – 68
MERIT-9: a patient information exchange guideline using
Michio Kimura a,*, Kazuhiko Ohe b, Hiroyuki Yoshihara c, Yutaka Ando d,
Fumiaki Kawamata e, Fumito Tsuchiya f, Hiroyuki Furukawa g, Shingo Horiguchi b,
Takaya Sakusabe h, Shigeki Tani a, Masanori Akiyama i
a Department of Medical Informatics, School of Medicine, Hamamatsu Uni6ersity, 3600 Handa Hamamatsu 431-3192, Japan
b Hospital Computer Center, The Uni6ersity of Tokyo, Tokyo, Japan
c Di6ision of Medical Information, Miyazaki Medical College, Miyazaki, Japan
d Department of Radiology, Keio Uni6ersity Hospital, Tokyo, Japan
e Otsuka Pharmaceutical Company Limited, Tokyo, Japan
f Di6ision of Pharmacy, Teikyo Uni6ersity Ichihara Hospital, Chiba, Japan
g Di6ision of Pharmacy, Kanazawa Uni6ersity Hospital, Kanazawa, Japan
h Weathernews Incorporated, Makuhari, Chiba, Japan
i International Medical Center of Japan, Tokyo, Japan
Received 20 February 1998; received in revised form 20 March 1998; accepted 28 March 1998
Abstract
To realize clinical data exchange between healthcare providers, there must be many standards in many layers.
Terms and codes should be standardized, syntax to wrap the data must be mutually parsable, then transfer protocolor exchange media should be agreed. Among many standards for the syntax, HL7 and DICOM are most successful. However, everything could not be handled by HL7 solely. DICOM is good for radiology images, but, other clinicalimages are already handled by other ‘lighter’ data formats like JPEG, TIFF. So, it is not realistic to use only onestandard for every area of clinical information. For description of medical records, especially for narrativeinformation, an standard generalized mark-up language, document type definition (SGML DTD) for medicalinformation, called MML (medical markup language) had been created in Japan. It is already implemented in morethan ten healthcare providers. However, it is again not realistic to use MML solely for clinical information in variouslevel of detail. Therefore, we proposed a guideline for use of available medical standards to facilitate clinicalinformation exchange between healthcare providers. It is called MERIT-9 (MEdical Records, Images, Texts,-Information eXchange). A typical use is HL7 messages, DICOM files, referred from an MML file in a patient record,as external entities. Both MML and MERIT-9 have been research projects of Japanese Ministry of Health and
* Corresponding author. Tel.: + 81 53 4352770; fax: + 81 53 4352769; e-mail: kimura@hama-med.ac.jp
1386-5056/98/$19.00 1998 Elsevier Science Ireland Ltd. All rights reserved. M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
Welfare and the purpose is to facilitate clinical data exchanges. They are becoming to be used in technicalspecifications for new hospital information systems in Japan. 1998 Elsevier Science Ireland Ltd. All rights reserved. Keywords: Medical data standard; Hospital information systems; Computerized medical record systems; Communitynetwork; Telemedicine
1. Introduction 2. What we can use now and what we still need?
It is needless to say that exchanging pa-
tients’ clinical information between health-
2.1. What we can use, for example, for
care facilities is very important. It is required
clinical obser6ation reporting
in many situations. Patient referrals betweenclinic and hospitals are the most frequent.
For syntaxes to wrap the observation data,
Then hospital may transfer information to/
from special examination laboratories, or to
[4], UN/EDIFACT [5], etc. A good compari-
other related healthcare service providers.
son between them is reported by S. From and
Any other facilities within allied healthcare
E. Brox [6]. After this survey, done by CEN
message format ENV 1613, for this purpose
[7]. In the United States, HL7 is now most
change, however, are different in each case.
widely and successfully used for this purpose.
Patient’s episode history is sent from clinics
HL7 now has six international affiliates.
to hospitals, while chemical laboratory com-
pany sends massive amount of lab test results
candidates include CPT-4 [8], and LOINC. In
Japan, The Japan Society of Clinical Pathol-
change, there must be a lot of agreementsbetween both sides. Fig. 1 shows what areneeded. First, a data transfer protocol, ormedia for off-line, should be agreed, to be atleast readable. Then, the syntax of a data fileshould be parsable for both of them, to knowwhat is where within the data file. In the caseof Fig. 1, HL7 [1] is used. Finally, the termsand codes in the expression should be under-standable. In Fig. 1, the left side usesJapanese lab test code while the counterpartuses LOINC [2]. Fortunately, thanks to amapping table between these codes, patient’sdata of gamma-GTP was transferred success-
Fig. 1. Clinical observation ‘gamma-GTP is 120’ is
transferred from database to database. For this, four
medical information, especially for the upper
layers of mutual understandings are needed. Item code,
syntax, data format and transfer method. M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
Fig. 2. Hierarchical structure of MML. ‘Clinical encounter section’ is described in detail. ‘Abbr.’ means this elementcould be abbreviated. ‘Rep.’ means multiplicity of this element. ‘MERIT-9’ in ‘Data type’ means this element is forexternal entity reference, described later.
mated data. Even though the syntax is now
LOINC. Thus, the code is mutually convert-
being brushed up by HL7 working group, it
is not the way that most ECG data areexchanged, until now. ECG vendors’ propri-
2.2. Wider co6erage is needed
etary data standards are mostly used, whichare deeply concerned with each vendor’s data
[10] for the part of clinical observation re-
porting. HL7 also covers orders of prescrip-
patient, which are captured by clinical en-
tions, nursing and intervention, etc. Looking
counters. It is not, however, the usual way to
describe and exchange this kind of informa-
orders and reports are what HL7 is mostly
tion between healthcare providers. The syn-
successful for descriptions of laboratory tests,
M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
prescription, etc. But, it is not suitable for
radiology examination orders are much more
descriptions of clinical signs, which are usu-
in detail, compared with the data varieties
ally described in texts of free format. We
offered by HL7. [11] Therefore, many locally
cannot solve everything by HL7 solely.
described elements had to be added, in orderto fetch usual physicians’ image examination
2.3. Variety of information granularity is
tions in each requirements for image quality.
HL7 has descriptions for radiology exami-
DICOM [12] is the most successful in this
nation orders. At Tokyo University Hospital,
HL7 is being used to transmit orders includ-
ing radiology examinations. Their implemen-
minor modifications on Supplement 8 Image
tation experiences made clear that, in Japan,
Storage Service Class and Supplement 10 Ba-sic Worklist Management Service Class [13]. In Japan, JIRA (Japan Industries associationfor Radiation Apparatus) translated DICOMdocuments in Japanese. It is often used andreferred in technical specifications for openbids of medical imaging systems in Japanesehospitals.
Even DICOM is so successful in radiology,
however, images other than radiological arecarried and archived by other image stan-dards, such as JPEG [14], TIFF [15], etc. even though DICOM committee has recentlyreleased a draft for specifications for visiblelight images [16]. Requirements for imagequality are different in many situations, froma 4000 × 4000 full 24 bit color to a 256 × 2568 bit grayscale. It is realistic for each imple-menter to select the best suitable solutionamong available candidates, which are men-tioned above.
Fig. 3. Original presumed case of uses of MERIT-9.
2.4. Meta information to help understanding
Case 1 is patient data transfer between hospital and
the episode sequentially is needed
clinic. It could be by floppy disk or on-line. In case 2,laboratory test company reports massive amounts oftest results to hospital. In this case, MML document
Most of the successful standards including
could be omitted. Then, the report consists of massive
HL7 files. In case 3 laboratory test controlling center
information messages. Therefore, they are for
collects lab test results of this area from many test sites.
clinical information captured in a certain
Case 4 shows that a patient wants to cumulate his/her
time. For HL7, it usually is one order or
examination history from many healthcare providers. In case 5, hospitals may like to use this for clinical case
result of examinations. For DICOM, it usu-
ally is for images of one image examination. M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
Fig. 4. An MML file refers an HL7 message as an external entity by a file name ‘A0001.HL7’. A DICOM file isreferred by a file name ‘D0002.DCM’.
As a result, it is very difficult to put one
Use of a hierarchical description for clinical
patient’s narrative episode which involves
MEDIX committee [19]. The idea is indispens-
diagnostic reports, bunch of prescriptions,
able, but, no detailed description of massive
data elements for clinical information ex-change has been published. CEN TC251 isnow also proposing, but not yet being unveiled
3. Medical markup language — an SGML
a standard for message of patient referral and
DTD for medical record information
As a consequence of the requirements men-
tioned in the succeeding chapter, a medical
prepared for now-realizing method of object
request brokering between healthcare infor-
in 1995, as a Japanese Ministry of Health and
mation systems. DICOM is already a standard
Welfare’s research project for electronic med-
based on objects concerning image examina-
ical records [17]. It is an SGML DTD (stan-
tions and HL7 version 3 is going to be on the
dard generalized mark-up language, document
same track. Therefore, this method of data
type definition) [18] for medical record infor-
description will be used for the basis of data
mation. As shown in Fig. 2, it is a hierarchy
transactions between them. As what is impor-
of descriptions of clinical information.
tant is not the data definition syntax, but the
What is in each data element, is described
structural definition of information, MML
by data types, which are similar to HISPP-
may not be using ‘mark-up’ descriptions of
information in future. Even then, it will still be
ing data types are used: ST; TS; ID; DT; and
used as a basis of clinical information descrip-
M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
Fig. 5. A DTD of an MML document which refers external HL7 messages designated as URI. File names are‘ca1001.hl7’ and ‘ca1002.hl7’, both under directory ‘pid001’. Minimal information (File type ( = HL72.3) andExamination date) from HL7 message contents are on DTD tag, in order to let DTD parser know what is in thereferred entity.
The research project of the Ministry is now
which are crisp and already successful stan-
in its third year. There are already more than
dards, for detailed specialty of information.
10 healthcare providers, from outpatient clin-ics to university hospitals, which are doingthe evaluations of this standard. 4. Patient information exchange guideline:
Total list of the data elements, a part of
which is shown in Fig. 2, is not very large,considering the required wide coverage. It is
possible to make a very precise and detailed
descriptions of the data elements for every
year later. It is to facilitate clinical informa-
type of orders, observations, etc. But it
tion exchange between healthcare providers.
makes the standard enormous and the enor-
Among many kinds of clinical information,
mous standard is very hard to be kept up-to-
laboratory test results, diagnostic images,
date in all part. Furthermore, there are many
prescriptions, are ready to be electronically
kinds of non-textual data required in clinical
information exchange. The typical example is
providers’ databases. It is because we have all
image data. Therefore, it is realistic to use
the necessities described in the Introduction
MML for narrative clinical information and
of this paper, for these three kinds of infor-
mation. Treatments, interventions will follow,
HL7 messages, DICOM files, TIFF files, etc.
then, diagnostic disease names. But, signs
M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
captured at clinical encounters are very hard
Tags for examination information associ-
to exchange in a electronically-recognizable
way. So the project concentrated on the top-
IS&C, because all others are just image
standards and have no information of clin-
Detailed understanding and usage of HL7,
change) is for exchanging lab test results,
prescriptions, images, as well as patient iden-
tification information, making full use of
External entity referring method. We de-
be referred from technical specifications for
cided on indirect pointing from directory
open bid of healthcare information systems.
Original presumed case of uses are shown in
Usually, by MERIT-9, a patient’s narrative
change media, transfer protocols, encrypting
episode is described by MML, with detailed
lab test results, prescriptions and diagnostic
uations in mind so that the best solution
TIFF files, etc. referred from MML file as
tion. Moreover, it is difficult to keep these
external entities. Recently, HL7 formed a
contents up-to-date. How external entities are
working group for SGML. It is preliminarily
intended to use SGML for an encoding rule
of HL7 messages. Thus, it is SGML withinHL7, while MERIT-9 proposes HL7 withinSGML. Fig. 4 shows the idea. 5. Differences of medical practice, illustrated
To realize clinical data exchange, the fol-
by using foreign standards
stated in the MERIT-9 standard. Listing of external entity repertoire: For
images; DICOM; IS&C [21]; JPEG; TIFF;
in countries outside Japan, except for MML.
presumed case of real use. Therefore, any
standard reflects customs of medical practice
Tags to be on the MML file representing
of the countries where it was created, more or
less. This time, by trying to use a foreign-
made standard, differences of medical prac-
tice between countries are clearly illustrated.
what is in the external entity, though not
We are reporting these things, thinking that
total details of inside. Therefore, minimal
they are helpful for future international stan-
dardization, as well as they are interesting.
and time, etc. should be on MML tags.
Generally speaking, doctors in Japan place
Detailed description of MML tags, keep-
(pharmacy, radiology, clinical laboratory)
M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
placing image examinations. Examination de-tails such as beam directions, contrast agent,
etc. are to be ordered in Japan, while they are
at the discretion of radiologists in the US.
Therefore, there are no fields for these data in
found one thing very common in Japan, but
is hard to be described by them. Single orders
which are to be reported as multiple individ-ual results, such as ‘Electrolytes’, ‘FBS (free
blood sugar) Glucose challenge test’, are han-dled as ‘batteries’. The variety of results are
determined by the examining laboratory. One
laboratory may report the latter as FBS be-
prescription in Japan. For example, they are
fore Glucose intake, 60 min after and 120
min after, while another laboratory may re-
prescription groups. In Japan, about 15% of
port it as before, 30, 60, 90 and 120 min. By
total prescriptions are powders. At Teikyo
HL7, when order placing, expected detail of
University Ichihara hospital, total number of
results cannot be described by them, unless
prescriptions in 1 day (1997/12/1) was 3745.
results of each timing were ordered individu-
ally. In Japan, however, these expected de-
usually have variety of different concentra-
tions. We had to find a way to specify this
information explicitly clear. Next, in Japan,
tee to give us a way to describe expected
macy, medicines to be taken at the sametiming (three times a day, two times a day,
one in the morning only, etc.) are grouped ina bag within the whole bag. So we had to put
information of prescription groups in order-
are not exclusive for medical images. This
ing messages. These small things were solved
means they are not reflecting each country’s
by ‘broader’ interpretation of existing fields
medical practice. From the beginning, when
international collaboration. As a result, DI-
segments. In the discussion to use HL7 for
COM is prepared to meet requirements at the
prescription in Japan, however, we thought
US, Europe and Japan, at the same time.
This is quite desirable and natural. It is be-
which are to be used for encoded order mes-
cause vendors of each side have certain mar-
‘Total daily dose’ while RXO doesn’t. In
Shimadzu are selling their products in US
Japan, prescription order is based on total
and Europe, while in Japan, we can buy GE,
daily dose. We write ‘Adalat-L three tabs,
after every meal, 7 days’ meaning ‘one tab for
each time, total 21 tabs’. Total is not 63
tablets. And this style of Total-daily-dose-
M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
based prescription is mandatory by law, for
Acknowledgements
our valid prescription orders. We requestedHL7 committee to add Total daily dose in
tion to following personnel for fruitful com-
By a survey at Teikyo University Ichihara
Hospital, total number of oral medications in
CareNet Inc., Dr Shigekoto Kaihara of Na-
tional Okura Hospital, Dr Hirozo Ueda and
Among them, 3100 had instruction of timing
Dr Yoshiyuki Matsumoto of the Ministry of
not associated with meals. This means 93% of
Health and Welfare, Professor Clem J. Mc-
total prescriptions has timings related with
Donald of Indiana University, Professor W.
meals. Usually, they are ‘after meals’, but
‘before meals’ (mostly Chinese traditional
medicine) ‘between meals’ ‘with meals’ are
not uncommon. Even for ‘after meals’, some-
sity, Dr Teruyoshi Hishiki of the University
times it is ‘after breakfast and dinner’, or
‘after breakfast and lunch’. In HL7 v2.3,
however, there is no description in this pre-
Chiba University, Dr Koichi Ishikawa of Na-
ciseness. We requested these detailed descrip-
tional Cancer Center, Mr Mitsuhiro Aizawa
of Arcobel Graphics Japan Inc., Mr HaruoKarasawa of Konica Corp., Mr Koichi Kitaof Toshiba Corp. 6. Final remarks
In the second year of the ministry project,
References
MERIT-9 is now being evaluated for its im-
[1] Health Level Seven, An application protocol for
plementations. It is adopted for technical spe-
electronic data exchange in health care environ-
cifications of national university hospital
ments. Version 2.3 Ann Arbor, MI, Health Level
information systems for clinical trail manage-
ment. Future expansions of applicable spe-
[2] A.W. Forrey, C.J. McDonald, G. De Moor, S.M.
cialties of information will be carried on
Huff, Logical observation identifier names andcodes (LOINC) database: a public use set of codes
according to the opinion described early in
and names for electronic reporting of clinical labo-
this thesis. However, these information like
ratory test results, Clin. Chem. 42 (1) (1996) 81 –
signs obtained by the clinical encounters
could be described in free text form, because
[3] ISO Standard, ASN.1. ISO 8824, 1987.
MML can have them in that form. Of course
[4] Euclides Consortium, Euclides Syntax Manual.
it is not transferable between databases in
[5] B.J. Love, UN EDIFACT-an EDI standard for
information retrievable manner, human clini-
healthcare, in: G.J.E. De Moor, C.J. McDonald
cians can read and understand the free text.
(Eds.), Progress in Standardization in Health Care
English version of information concerning
Informatics, ISO Press, 1993, pp. 156 – 161.
[6] S. From, E. Brox, Investigation of syntaxes for
existing interchange formats to be used in health-
the Japan Association of Medical Informat-
care, in: G.J.E. De Moor, C.J. McDonald (Eds.),
ics, research committee for MML/MERIT-9.
Progress in Standardization in Health Care Infor-
matics, ISO Press, 1993, pp. 118 – 126. M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
[7] Comite Europeen de Normalisation. CEN ENV
[16] Digital Imaging and Communications in Medicine
1613: Messages for Exchange of Clinical Labora-
(DICOM), NEMA Publications PS 3. Supplement
tory Information. Brussels: CEN, 1994.
15: Visible Light Image and Anatomic Frame of
[8] CPT-4, Clinical Procedures and Terminologies,
Reference for Endoscopy, Microscopy and Pho-
American Medical Association, Chicago, II, 1987.
tography. Draft for Public Review. The National
[9] Committee of Laboratory Codes and Laboratory
electrical Manufacturers Association, Rosslyn VA,
Instruments, The Japan Society of Clinical Pathol-
ogy, Classification and Coding for Clinical Labo-
[17] T. Hishiki, K. Ohe, H. Yoshihara, M. Kimura, Y.
ratory Tests (JLAC9 release 2). Rinsho Byori
Ando, T. Sakusabe, F. Kawamata, R. Yamamoto,
S. Yamazaki, Y. Hirose, K. Ohashi, K. Matsui, K.
[10] American Society for Testing and Materials,
Minagawa, Medical Markup Language: A simple
method for clinical data exchange, Proceedings of
Transferring Clinical Observations Between Inde-
The Third International Conference on the Medi-cal Aspects of Telemedicine, 1997, pp. 117.
pendent Computer Systems, Philadelphia, PA,
[18] N. Bradley, The Concise SGML Companion, Ad-
[11] K. Ohe, S. Kaihara, Implementation of HL7 to
[19] J.J. Harrington, T.J.R. Benson, A.L. Spector,
client – server hospital information system (HIS) in
IEEE P1157 Medical Data Interchange (MEDIX)
the University of Tokyo Hospital, J. Med. Syst. 20
Committee: Overview and Status Report, Proceed-
ings of the Fourteenth Symposium on Computer
[12] Digital Imaging and Communications in Medicine
(DICOM), NEMA Publications PS 3.1-3.12, The
[20] M. Kimura, Telemedicine Information Standards
National electrical Manufacturers Association,
in Japan, Proceedings of the Third International
[13] H. Gnoyke, Standards for the integration of
modalities with information system and IMAC
[21] M. Kimura, N. Ohyama, K. Inamura, Y. Ando,
N. Shigemura, Y. Shima, T. Saito, IS&C (Image
ments, Proceedings of Medical Imaging 1996,
Save and Carry) Standard: Standardized Exchange
PACS Design and Evaluation, vol. 2711, SPIE,
Media for Medical Information, Proceedings of
the Eighth World Congress on Medical Informat-
[14] C-Cube Microsystems, JFIF: JPEG File Inter-
ics (MEDINFO-95), 1995, pp. 207 – 211.
change Format version 1.02, Milipitas, CA, 1992.
[22] ISO/IEC JTC1/ SC29, MPEG: Information Tech-
[15] Aldus Developers Desk, TIFF Revision 6.0 Final,
nology-Generic Coding of Moving Pictures and
Aldus Corporation, 441 First Ave. South, Seattle,
RELATÓRIO DE ENTRADA DE PRODUTOS - PRODUTOS--------------------------------------------------------------------------------------------------------------------------------------------------------- NOTA: 613674---------------------------------------------------------------------------------------------------------------------------------------------------------CODIGO PRODUTO--------------------
Prevention of human to human transmission Swine flu spreads between humans through coughing or sneezing and people touching something with the virus on it and then touching their own nose or mouth. Swine flu cannot be spread by pork products, since the virus is not transmitted through food. The swine flu in humans is most contagious during the first five days of the illness although some peop
 International Journal of Medical Informatics 51 (1998) 59 – 68
MERIT-9: a patient information exchange guideline using
Michio Kimura a,*, Kazuhiko Ohe b, Hiroyuki Yoshihara c, Yutaka Ando d,
Fumiaki Kawamata e, Fumito Tsuchiya f, Hiroyuki Furukawa g, Shingo Horiguchi b,
Takaya Sakusabe h, Shigeki Tani a, Masanori Akiyama i
a Department of Medical Informatics, School of Medicine, Hamamatsu Uni6ersity, 3600 Handa Hamamatsu 431-3192, Japan
b Hospital Computer Center, The Uni6ersity of Tokyo, Tokyo, Japan
c Di6ision of Medical Information, Miyazaki Medical College, Miyazaki, Japan
d Department of Radiology, Keio Uni6ersity Hospital, Tokyo, Japan
e Otsuka Pharmaceutical Company Limited, Tokyo, Japan
f Di6ision of Pharmacy, Teikyo Uni6ersity Ichihara Hospital, Chiba, Japan
g Di6ision of Pharmacy, Kanazawa Uni6ersity Hospital, Kanazawa, Japan
h Weathernews Incorporated, Makuhari, Chiba, Japan
i International Medical Center of Japan, Tokyo, Japan
Received 20 February 1998; received in revised form 20 March 1998; accepted 28 March 1998
Abstract
International Journal of Medical Informatics 51 (1998) 59 – 68
MERIT-9: a patient information exchange guideline using
Michio Kimura a,*, Kazuhiko Ohe b, Hiroyuki Yoshihara c, Yutaka Ando d,
Fumiaki Kawamata e, Fumito Tsuchiya f, Hiroyuki Furukawa g, Shingo Horiguchi b,
Takaya Sakusabe h, Shigeki Tani a, Masanori Akiyama i
a Department of Medical Informatics, School of Medicine, Hamamatsu Uni6ersity, 3600 Handa Hamamatsu 431-3192, Japan
b Hospital Computer Center, The Uni6ersity of Tokyo, Tokyo, Japan
c Di6ision of Medical Information, Miyazaki Medical College, Miyazaki, Japan
d Department of Radiology, Keio Uni6ersity Hospital, Tokyo, Japan
e Otsuka Pharmaceutical Company Limited, Tokyo, Japan
f Di6ision of Pharmacy, Teikyo Uni6ersity Ichihara Hospital, Chiba, Japan
g Di6ision of Pharmacy, Kanazawa Uni6ersity Hospital, Kanazawa, Japan
h Weathernews Incorporated, Makuhari, Chiba, Japan
i International Medical Center of Japan, Tokyo, Japan
Received 20 February 1998; received in revised form 20 March 1998; accepted 28 March 1998
Abstract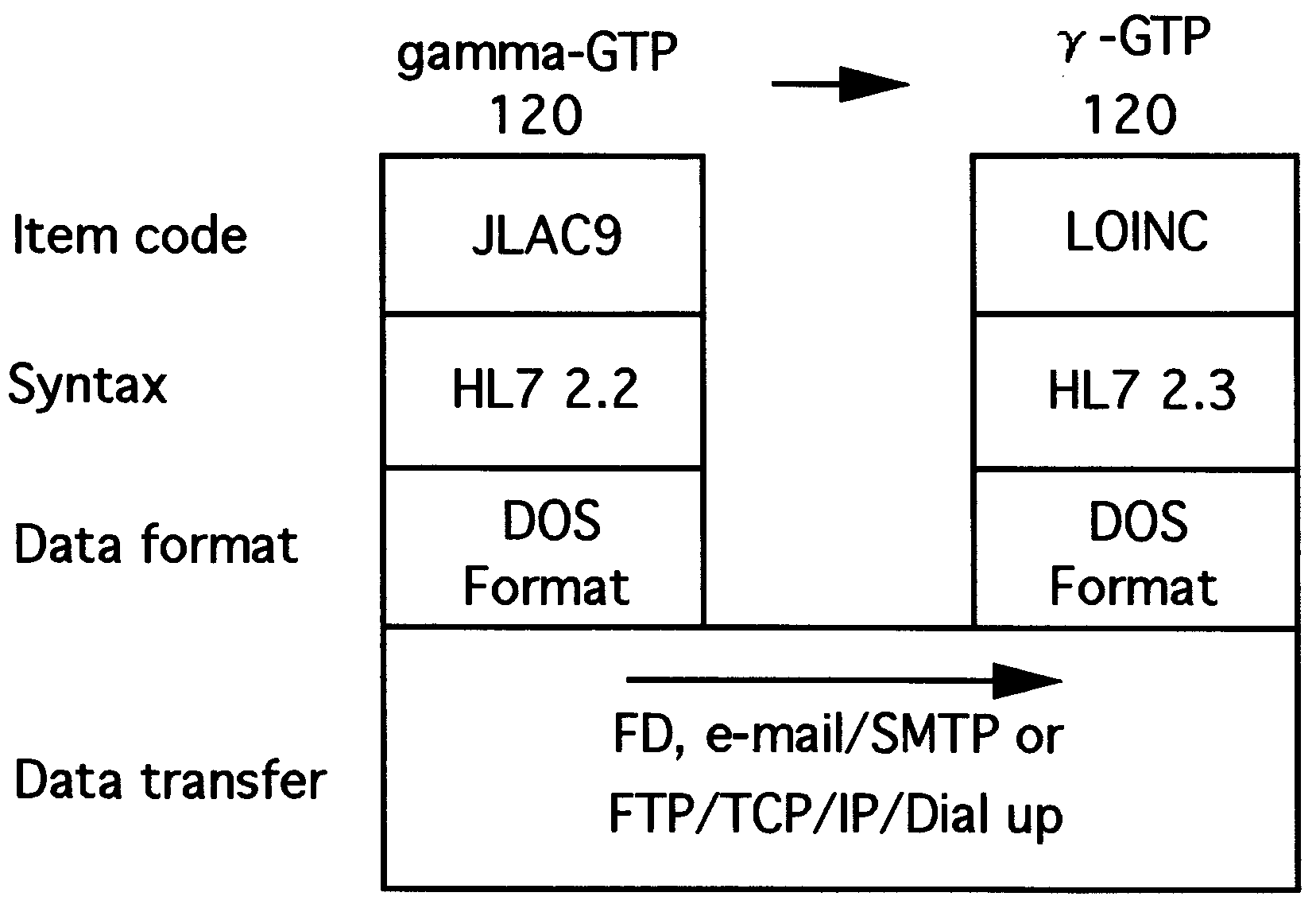 M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
Welfare and the purpose is to facilitate clinical data exchanges. They are becoming to be used in technicalspecifications for new hospital information systems in Japan. 1998 Elsevier Science Ireland Ltd. All rights reserved.
M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
Welfare and the purpose is to facilitate clinical data exchanges. They are becoming to be used in technicalspecifications for new hospital information systems in Japan. 1998 Elsevier Science Ireland Ltd. All rights reserved.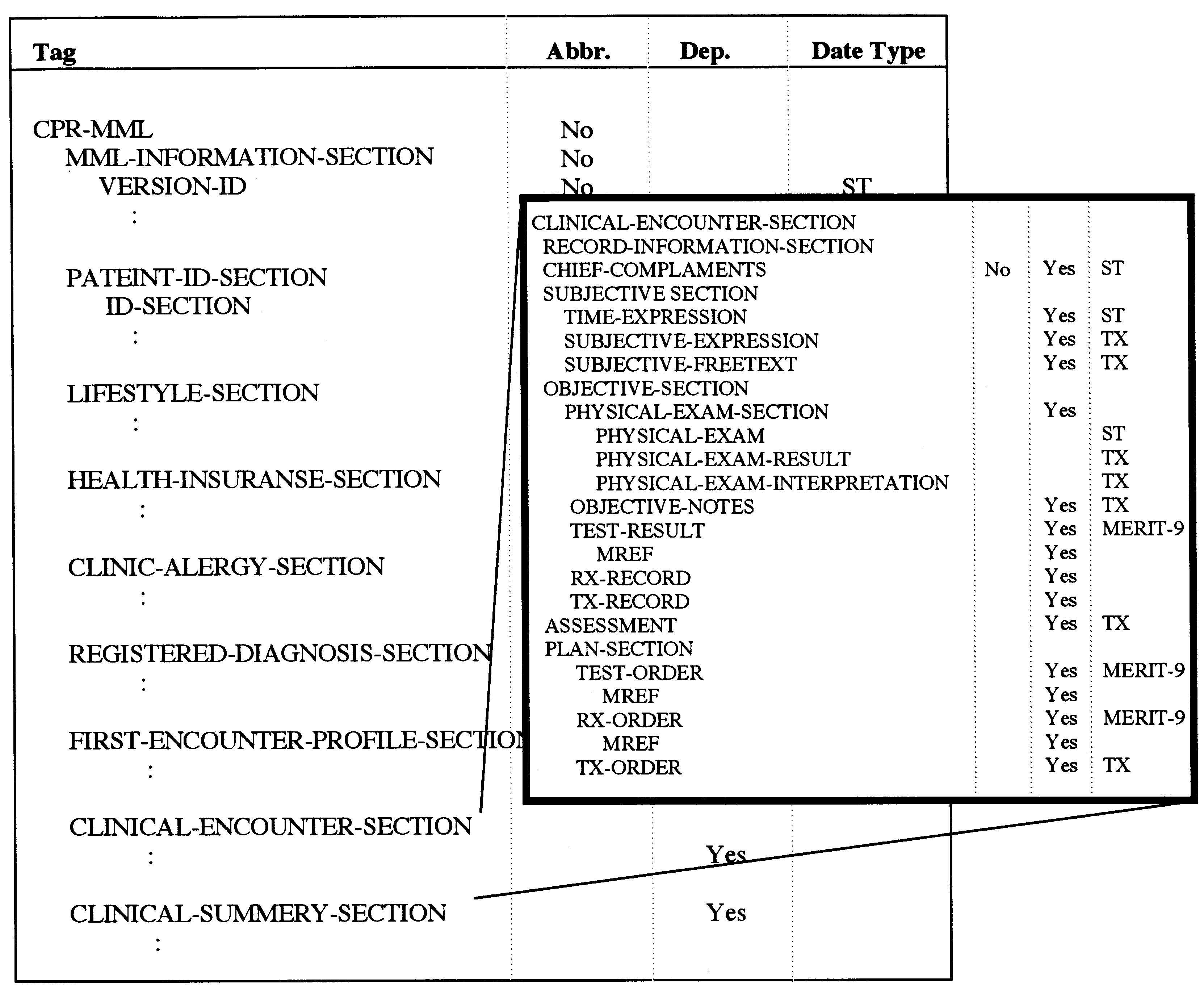 M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
Fig. 2. Hierarchical structure of MML. ‘Clinical encounter section’ is described in detail. ‘Abbr.’ means this elementcould be abbreviated. ‘Rep.’ means multiplicity of this element. ‘MERIT-9’ in ‘Data type’ means this element is forexternal entity reference, described later.
M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
Fig. 2. Hierarchical structure of MML. ‘Clinical encounter section’ is described in detail. ‘Abbr.’ means this elementcould be abbreviated. ‘Rep.’ means multiplicity of this element. ‘MERIT-9’ in ‘Data type’ means this element is forexternal entity reference, described later.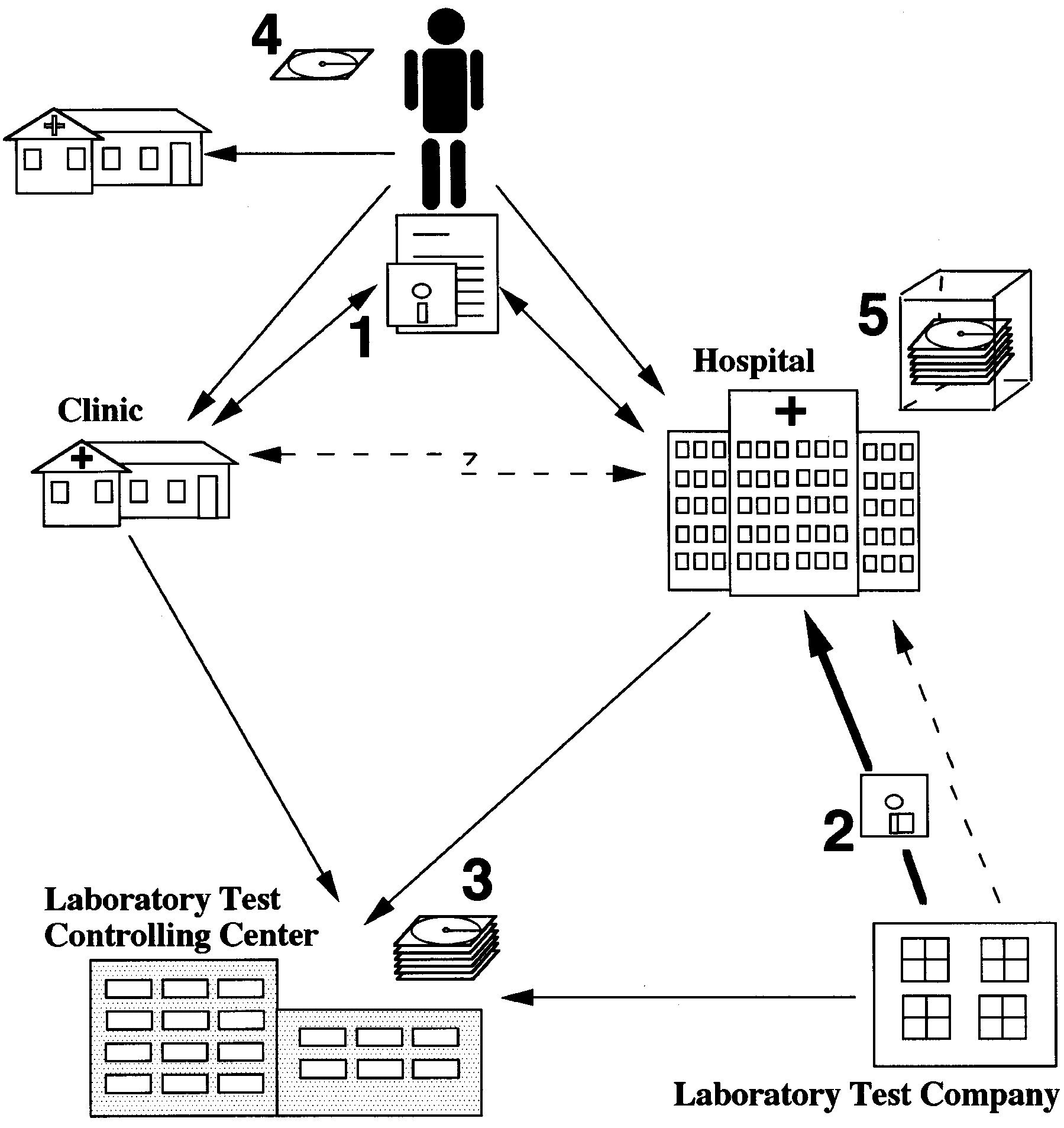 M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
prescription, etc. But, it is not suitable for
radiology examination orders are much more
descriptions of clinical signs, which are usu-
in detail, compared with the data varieties
ally described in texts of free format. We
offered by HL7. [11] Therefore, many locally
cannot solve everything by HL7 solely.
M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
prescription, etc. But, it is not suitable for
radiology examination orders are much more
descriptions of clinical signs, which are usu-
in detail, compared with the data varieties
ally described in texts of free format. We
offered by HL7. [11] Therefore, many locally
cannot solve everything by HL7 solely.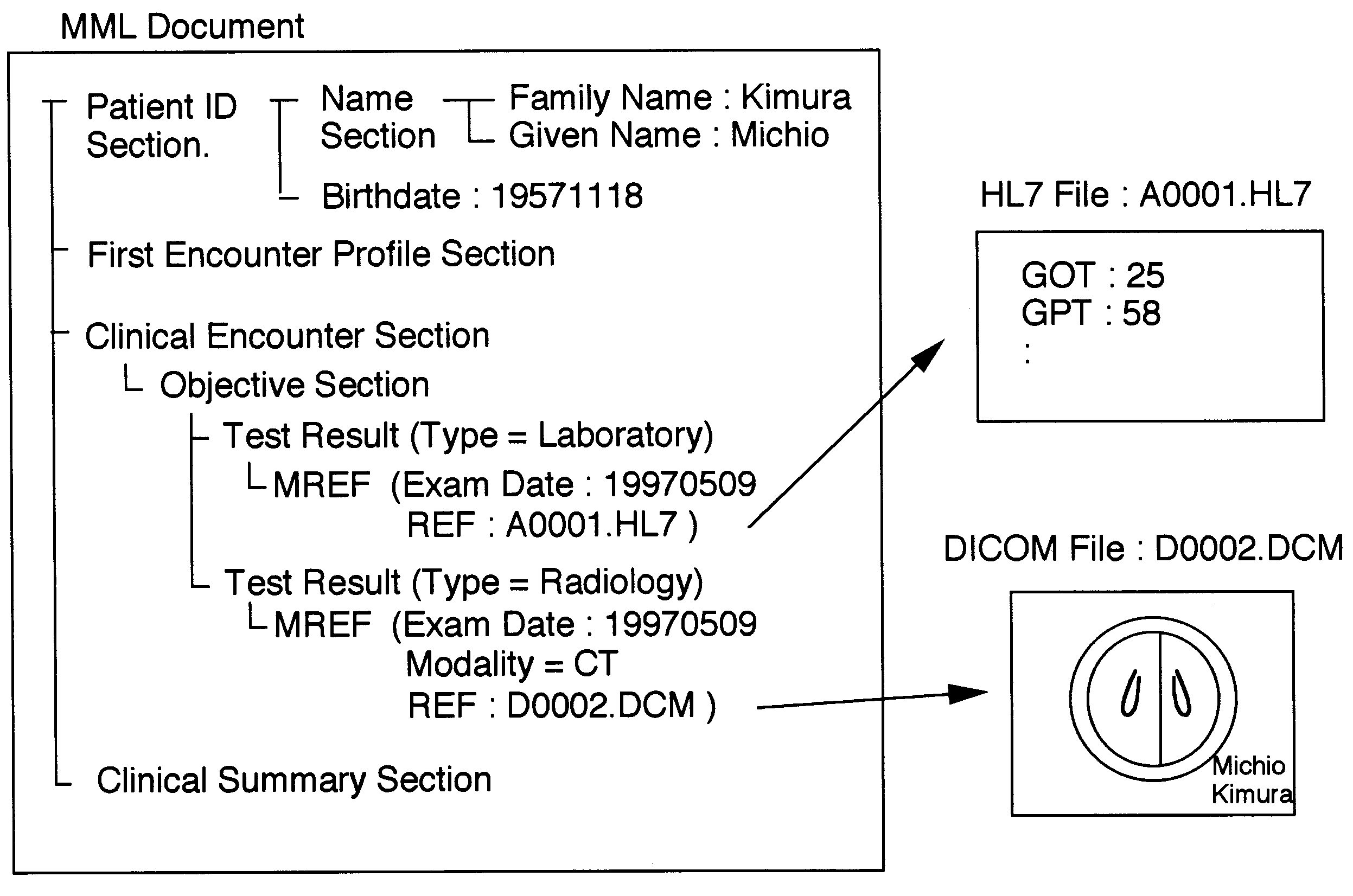 M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
Fig. 4. An MML file refers an HL7 message as an external entity by a file name ‘A0001.HL7’. A DICOM file isreferred by a file name ‘D0002.DCM’.
M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
Fig. 4. An MML file refers an HL7 message as an external entity by a file name ‘A0001.HL7’. A DICOM file isreferred by a file name ‘D0002.DCM’.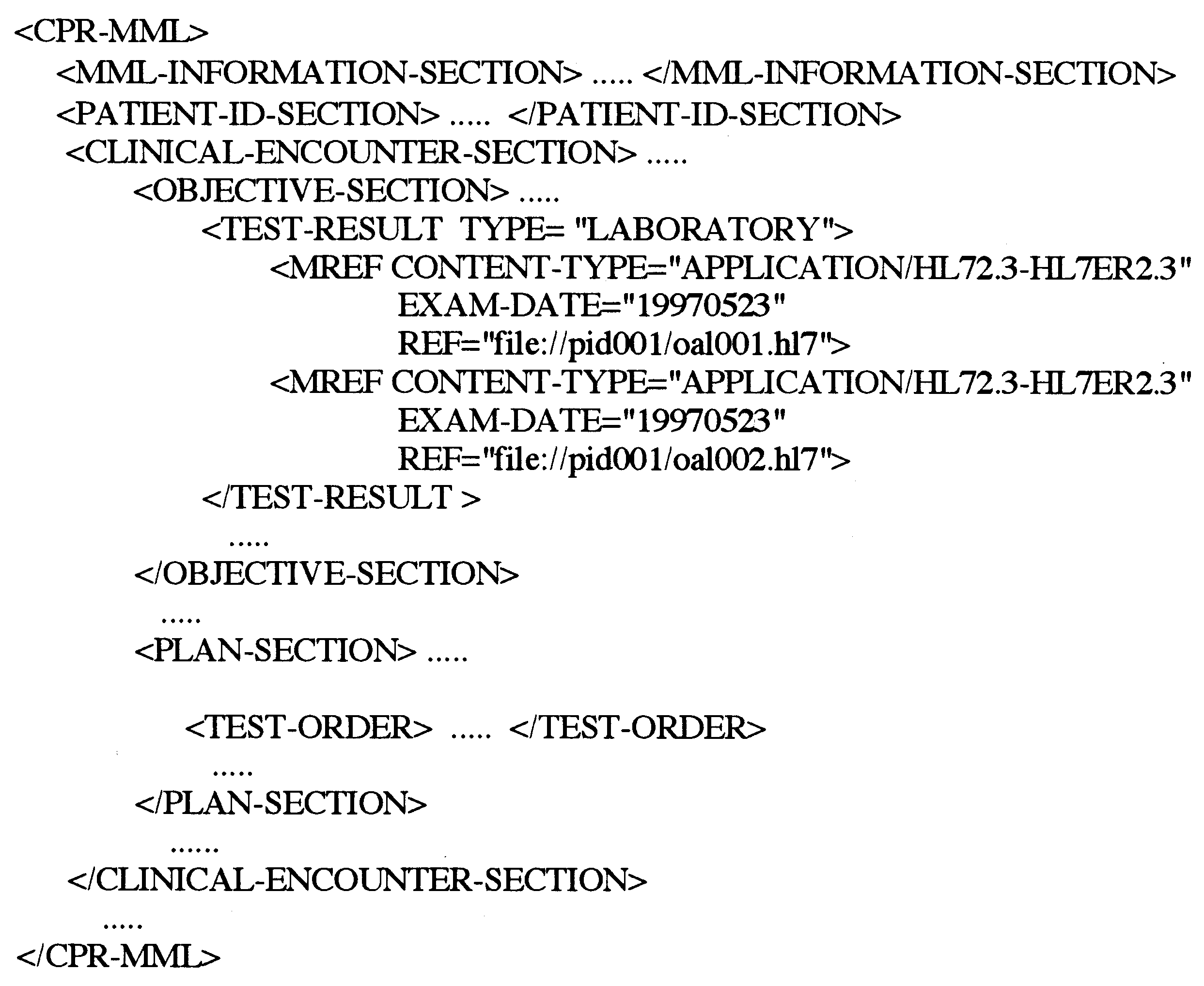 M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
Fig. 5. A DTD of an MML document which refers external HL7 messages designated as URI. File names are‘ca1001.hl7’ and ‘ca1002.hl7’, both under directory ‘pid001’. Minimal information (File type ( = HL72.3) andExamination date) from HL7 message contents are on DTD tag, in order to let DTD parser know what is in thereferred entity.
M. Kimura et al. / International Journal of Medical Informatics 51 (1998) 59 – 68
Fig. 5. A DTD of an MML document which refers external HL7 messages designated as URI. File names are‘ca1001.hl7’ and ‘ca1002.hl7’, both under directory ‘pid001’. Minimal information (File type ( = HL72.3) andExamination date) from HL7 message contents are on DTD tag, in order to let DTD parser know what is in thereferred entity.