MEDICINE Screening for the obstructive sleep apnea syndrome among guards in alternating work shifts Sleep Diagnostics & Therapy Center of the Central Military Hospital of the Hungarian Army,This study was conducted to appraise the prevalence of OSAS among individuals employed in alternating work shifts. The tentative diagnosis suggested by screening was validated by testing in a sleep laboratory; afflicted individuals received appropriate treatment and follow-up care. Screening conducted by administering a questionnaire suggested OSAS in 23 per cent of 218 subjects employed as sentries/guards in alternating work shifts. Individuals identified by screening underwent polysomnography in a sleep diagnostics laboratory in order to confirm the tentative diagnosis. Advanced OSAS is associated with abnormal enhancement of daytime sleepiness, which results in significant impairment of attention, mental concentration, vigilance, cognitive and job performance in afflicted individuals employed in alternating work shifts.Introduction
Chronic daytime sleepiness is an extremely common complaint that reduces the quality of life substantially. It interferes with mental functioning and performance through a complicated mechanism. Frequently, it is a potential cause of fatality resulting from industrial or accidents. The underlying causes of chronic daytime sleepiness include primary sleep disorders (such as obstructive sleep apnea, sleep-related motor disorders, narcolepsy, idiopathic hypersomnia, abnormalities of the circadian rhythm of sleep/wakefulness), neurological and psychiatric conditions resulting in somnolence, a variety of internal diseases, drug effects, as well as further forms of chronic sleep insufficiency. Although it is not possible to rank underlying causes according to their relative frequency, multiple causes of chronic daytime sleepiness can be and should be sought for in any given patient. An outstanding example of these is obstructive sleep apnea syndrome (OSAS), a disorder of public health significance. The characteristic symptoms of OSAS are summarized in Table 1. Analyzing the statistics of OSAS patients and healthy controls, a significant relationship has been demonstrated between accidents caused by falling asleep and obstructive apnea.1 ARBUS explored the nature of the disorders of sleep and alertness among 110 drivers (aged 28 to 57 years) who have
Address for correspondence:ZOLTÁN SZAKÁCSCentral Military Hospital of the Hungarian ArmySleep Diagnostics & Therapy, Budapest, HungaryE-mail: alvas@axelero.hu
Z. SZAKÁCS & P. KÖVES: Obstructive sleep apnea syndrome
caused severe road accidents because of falling asleep.2 Involuntary sleep resulted from obstructive sleep apnea in 31 per cent, from shift work in 38 per cent, and from narcolepsy in 10 per cent of these individuals. In a further 12 per cent of cases, prolonged use of tranquilizers with a long half-life was the likely cause of the accident. The prevalence of OSAS is 4 per cent in the general population. Among males, however, it is 8 to 12 per cent in the age group between 40 to 60 years, and it is as high as 15 to 20 per cent among men older than 60 years of age. More than 30 per cent of hypertensive patients is afflicted also by undiagnosed OSAS – and in almost 70 per cent, nocturnal hypoxic stress is the underlying cause of unrelenting hypertension.3–8 OSAS augments mortality from stroke and myocardial infarction 7- to 10-fold; it also increases the incidence of industrial and road accidents 8- to 10-fold.9–14
Table 1. Clinical manifestations of obstructive sleep apnea syndrome (OSAS)
Principal manifestations
1. Enhanced daytime drive to sleep/somnolence2. Abnormal snoring
Common signs & symptoms
1. Disturbed sleep2. Nocturnal enuresis3. Symptoms of cognitive deficit 4. Irritability, personality changes5. Reduced performance, easy fatigability6. Impaired mental concentration7. Irritability, disposition for depression 8. Prolonged awakening, obtundation or confusion9. Morning headache
10. Morning dry mouth11. Feeling unrefreshed after a night’s sleep12. Excessive, coarse jerking (of extremities and torso) during sleep
Manifestations suggestive of the severity of the clinical condition
1. Pronounced daytime sleepiness2. Nocturnal (diurnal) cardiac arrhythmia3. Cor pulmonale4. Awake hypercapnia/hypoxia5. Polycythemia6. Pathologic obesity
Evidently, shift workers are at an enhanced risk of experiencing daytime sleepiness
and symptoms of mental deficit. Among these individuals, patients with organic sleep disorders are especially jeopardized by consequential industrial accidents and errors
Z. SZAKÁCS & P. KÖVES: Obstructive sleep apnea syndrome
resulting from attention deficit at job. Evidently, the insomnia-hypersomnia syndrome caused by the derangement of circadian rhythm is complicated in such cases by sleep fragmentation and hypersomnia. The latter result in severe and chronic daytime sleepiness, mental deficit, as well as the decline of attention, long-term memory, and executory functions.15,16
This study was conducted to appraise the prevalence of OSAS among individuals
employed in alternating work shifts. Identified cases were validated by testing in a sleep laboratory; afflicted individuals received appropriate treatment and follow-up care.
The study population comprised 218 shift workers employed as sentries/guards. The
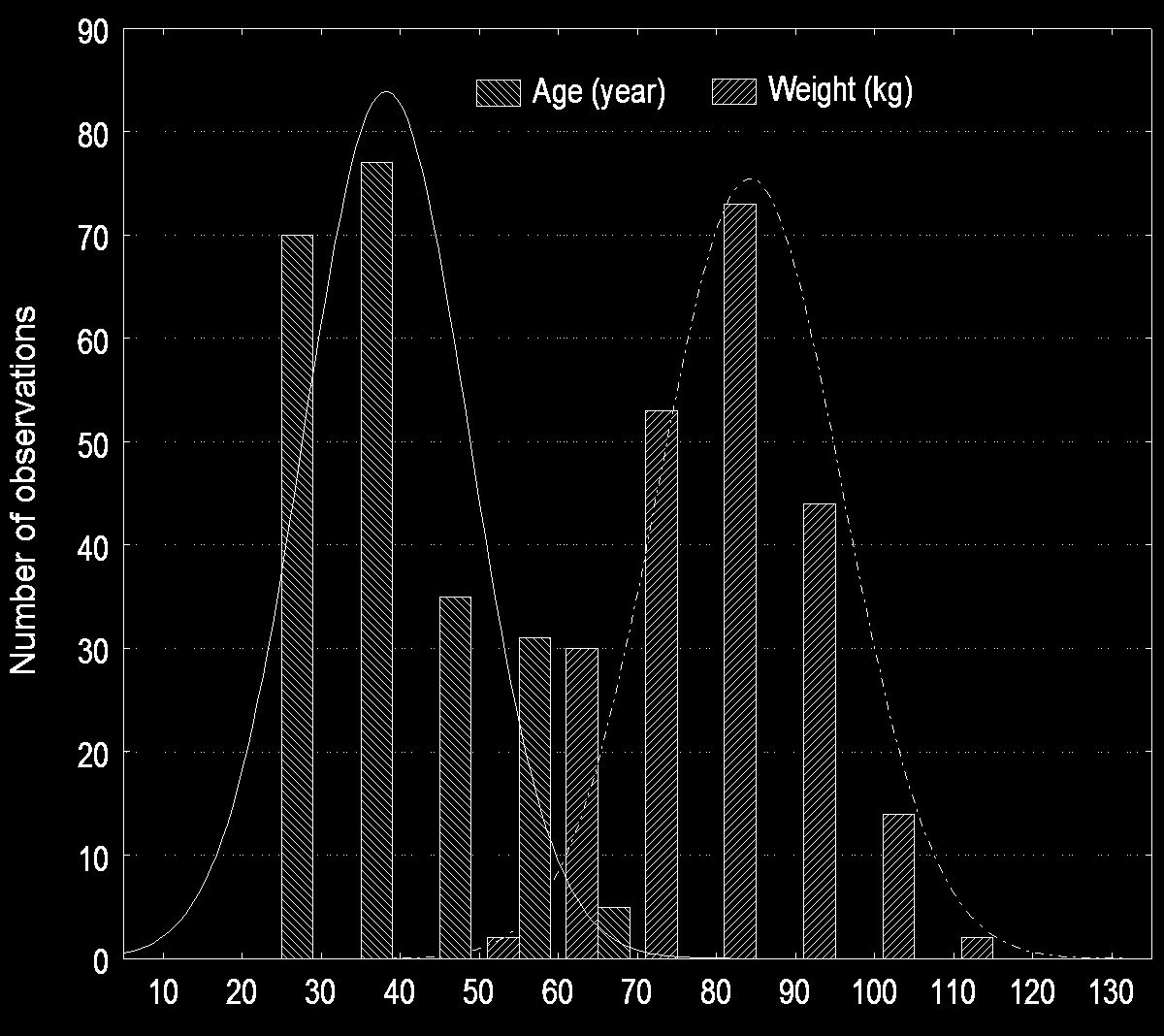
tentative diagnosis of OSAS was established and the presence of its complications ascertained by screening. This was undertaken using a questionnaire developed by the Sleep Diagnostics Center of the HA Central Military Hospital and field-tested in two epidemiological studies conducted in Hungary.17 The items, grouped in the questionnaire were assorted to yield composite variables reflecting the severity of daytime sleepiness and attention deficit, the risk of nocturnal snoring (hypertension, diabetes, cardiac-cerebrovascular events) in order to substantiate the tentative diagnosis of OSAS. All the studied subjects were males; their age (mean: 38.05 year, SD: 10.36). and weight (mean: 83.84 kg, SD: 11.52) distribution is shown by Figure 1. The only realistic expectation from screening with a questionnaire is to identify suspect cases. The efficacy of screening is greatly dependent on the contents and structure of the questionnaire; the organization of the screening effort; and the dedication of screening staff. Establishing the final diagnosis belongs to the competence of the sleep diagnostics laboratory. The latter is to clarify the nature of the disorder and to recognize its complications; as well as to evaluate the clinical severity of OSAS (through the joint appraisal of sleep laboratory parameters, clinical manifestations and subjective symptoms) – all these are determinants of the therapeutic approach. Standard polysomnography is an essential method for studying primary sleep disorders. Testing was done with Alice 3 and 4 equipment (Respironics Co.). Respiratory movements were monitored with a Pro-Tech Piezo Respiratory Effort sensor, whereas oronasal airflow was measured with Stardust Nasal Cannulae. Pulse oximetry was used to follow changes in the oxygen saturation of the blood (SaO2), along with the ECG monitoring of cardiac rhythm. Polysomnographic recordings comprised electroencephalographic (EEG) tracings (of C4A2 and C3A2 leads), electro-oculogram (EOG), and submental electromyogram (EMG). Apnea was defined as the cessation of oronasal airflow for at
Z. SZAKÁCS & P. KÖVES: Obstructive sleep apnea syndrome
least 10 seconds. Hypopnea was identified as an at least 50-per-cent reduction in the amplitude of airflow for a minimum of 10 seconds and/or leading to a 4-per-cent reduction in SaO2, or precipitating physiological arousal (alpha-activity for 3 seconds at least). The apnea/hypopnea index (AHI) was calculated as the mean of cumulative apneic and hypopneic episodes occurring per hour of sleep.
Figure 1. Age and weight distribution of the study population
According to current diagnostic principles, an AHI of >30 events/hour reflects
severe OSAS, whereas moderate and mild disease is identified by an AHI of >15 to <30 events/hour and >5 to <15 events/hour, respectively.
Z. SZAKÁCS & P. KÖVES: Obstructive sleep apnea syndrome
Results of screening
Table 2 shows the distribution of essential symptoms and of complications among the OSAS patients identified by screening. The latter – implemented using a questionnaire – suggested reasonable suspicion of OSAS in 3%, probable OSAS in 20%, and largely ruled out OSAS in 77% of the study population. On the base of the questioner score, we divided the subjects three groups: between 0–168 points OSAS unlikely, between 169–299 points OSAS presumable and between 270–336 points OSAS reasonably suspected. The sensibility of the questionnaire is 90.8%, specificity: 72.8%, positive predictive value: 83.9% and negative predictive value: 83.5%. Special attention was devoted to bypassing the waiting list of subjects scheduled for testing in the sleep laboratory if reasonably suspected OSAS was accompanied by potentially dangerous complications.
Table 2. The distribution of OSAS suspects identified by screening with the questionnaire
category number of subjects percentage OSAS unlikely OSAS presumable OSAS reasonably suspected
Figure 2. Comorbidity associated with OSAS
Z. SZAKÁCS & P. KÖVES: Obstructive sleep apnea syndrome
Among the 50 patients with suspected OSAS, 6% were hypertensive, 6% diabetic,
58% over-weight and 70% complained of mental deficit symptoms. A history of a cardiac-cerebrovascular event and of a road accident resulting from falling asleep were identified in 4–4% of these subjects (Figure 2). Results of testing in the sleep laboratory
Forty-seven subjects underwent testing in the sleep diagnostics laboratory. Scheduling was based on disease severity – patients with reasonably suspected OSAS had priority. Non-compliance was expected to be low and indeed, only 3 of the 50 patients with reasonably suspected OSAS declined polysomnographic testing. It is nevertheless convincing that the majority of subjects with distressing signs and symptoms readily subjected themselves to sleep testing – regardless of potential hindrances.
Fifteen of the 47 subjects had severe and 13 had moderate or mild OSAS. Other
forms of sleep-related respiratory disorders were identified in 14 individuals. One patient had sleep-related motor disorder, whereas four were diagnosed with unidentified forms of sleep-awake disorder (Figure 3).
Figure 3. Diagnostic polysomnography findings of 47 patients with reasonably suspected OSAS
Z. SZAKÁCS & P. KÖVES: Obstructive sleep apnea syndrome
Polysomnography revealed the following as typical characteristics of patients with
1. The proportion of the duration of slow wave sleep to the total duration of sleep
was 10.9±2.8% (normal range: 16 to 26%).
2. Microarousals, potentially related to pathogenic episodes of sleep-dependent
respiration: 39.5±13.6 events/hour (normal range: 0 to 20 events/hour).
3. Multiple sleep latency test (MSLT – an objective index of daytime sleepiness):
7.8±3.4 minute (an MSLT <10 minutes is considered obviously abnormal). Outcome of therapy
Individual cases of any disorder are characterized by unique combinations of disease features – this is particularly true for OSAS. Meticulous depiction, that is, portrayal of singular features is a prerequisite to individualized management that holds out the hope of lasting therapeutic efficacy.
The following factors should be considered when designing the individualized
• The existence of any obvious anatomical abnormality should be ruled out.
• The presence of underlying disorders (e.g. hyper- or hypothyroidism,
acromegaly, etc.) as potential causes of OSAS should be checked.
• The severity of the disease should be appraised:
– typical clinical manifestations (excessive daytime sleepiness, morning headache
and obtundation, inflammatory disorders of the upper airways, morning drymouth, hypertension, personality changes, memory impairment) should becharacterized;
– dangerous complications suggestive of advanced disease (e.g. prominent
daytime sleepiness, cor pulmonale, cardiac arrhythmia, awake hypoxia orhypercapnia, polycythemia, historical progression, stroke, myocardialinfarction, accident-proneness) should be identified;
– the results of polysomnography and electrophysiologic testing (apnea index,
lowest SaO2, sleep latency) should be interpreted.
• Thorough assessment, as well as the careful judgement of expected benefits and
potential risks of therapy can yield a therapeutic approach appropriate for any given case.
As regards our patient population, lifestyle changes and pharmacotherapy have been
elected for mild OSAS. The former comprised health education in sleep hygiene, targeted weight reduction, complex training (including mental guidance), and
Z. SZAKÁCS & P. KÖVES: Obstructive sleep apnea syndrome
restrictions on medication use. SSRIs, fluoxetine, cilasapril, and theophylline were administered as drug therapy. In moderate OSAS, these two treatment modalities have been supplemented with mechanical intervention (intraoral prostheses and CPAP), whereas CPAP was the mainstay of the management of severe OSAS.
Mechanical therapy was implemented using the CPAP device (a BIPAP machine
was used only during the initial period of treatment). The effective pressure setting in the sleep laboratory was done in 11 of the 15 patients with severe OSAS. Treatment with a CPAP device was justified in 8 of these cases; in compliance with the pertinent principles of the profession, these patients are still being followed up.
Discussion
Excessive daytime sleepiness (EDS) is a common manifestation of the obstructive sleep apnea syndrome and it is an outstanding risk factor of industrial and road accidents. Our survey conducted using a questionnaire suggested OSAS in 23 per cent of 218 shift workers (employed as sentries/guards). Suspect cases were subjected to testing in a sleep laboratory; polysomnography confirmed the tentative diagnosis. Based on literature data, OSAS was rated severe if the apnea/hypopnea index was higher than 30 events/hour. The extent of daytime sleepiness was measured with the multiple sleep latency test, performed in the sleep laboratory. Our subjects with OSAS of variable severity have been started on appropriate therapy and are being followed up continuously.
Severe OSAS is characterized by an excessive increase in daytime sleepiness. When
employed for shift work, patients with this disorder experience a substantial decline of attention, concentration, vigilance, job and cognitive performance – compared to their healthy colleagues. The relationship between sleep-dependent respiratory disorders and manifestations of neurophysiological deficit has been most thoroughly explored by the Wisconsin Sleep Cohort Study. A total of 841 employees were investigated during the night hours by polysomnography. Multiple regression analysis of results demonstrated a negative correlation between the apnea/hypopnea index and psychomotor performance.18 Appropriate therapy corrects these defects, eliminates sleepiness, and improves performance.19 Shift workers suffering from primary sleep disorders (OSAS, narcolepsy, restless leg syndrome) should be considered a poor-risk group as regards industrial accidents.20 Identifying sleep-related respiratory abnormalities is important not only for afflicted patients, but also for the prevention of industrial and road accidents, as well as of errors resulting from inattention and daytime sleepiness.21
Z. SZAKÁCS & P. KÖVES: Obstructive sleep apnea syndrome
References
1. C. F. GEORGE: Driving and automobile crashes in patients with obstructive sleep apnoea/hypopnoea
syndrome. Thorax, 59 (2004) 804–807.
2. E. KLEIN, D. KOREN, I. ARNON: No evidence of sleep disturbance in post-traumatic stress disorder: a
polysomnographic study in injured victims of traffic accidents. Isr. J. Psychiatry Relat. Sci., 39 (2002) 3–10.
3. P. LAVIE: Sleep apnea in industrial workers in San Marino population. In: C. GUILLEMINAULT, E.
LUGARESI (Eds), Sleep/Wake Disorders. Natural History, Epidemiology, Long term Evolution. New York Raven Press, 1983, pp. 127–135.
4. A. SASSANI, L. J. FINDLEY, M. KRYGER: Reducing motor-vehicle collisions, costs, and fatalities by
treating obstructive sleep apnea syndrome. Sleep, 27 (2004) 453–458.
5. T. YOUNG, M. PALTA, J. DEMPSEY: Occuerence of sleep disordered breathing among middle-aged
adults. N. Engl. J. Med., 328 (1988) 1230–1235.
6. H. M. KRYGER, R. ROOS, K. DELAINE: Utilization of health care servicies in patients with severe
obstructive sleep apnea. Sleep, 19 (1996) 111–117.
7. V. HOFFSTEIN, I. RUBINTSTEIN, S. MATEIKA: Determinants of blood pressure in snorers. Lancet, 2
8. M. E. HOWARD, A. V. DESAI, R. R. GRUNSTEIN: Sleepiness, Sleep Disordered Breathing and Accident
Risk Factors in Commercial Vehicle Drivers. Am. J. Respir. Crit. Care Med., 39 (2004) 258–262.
9. S. A. TZEMENTZIS, J. S. GILLA, E. R. HITCHKOCK: Diurnal variation and activity during the onset of
stroke. Neurosurgery, 17 (1985) 901–904.
10. C. BASSETTI, M. S. ALDRICH: Sleep apnea in acute cerebrovascular disease. Sleep, 22 (1999) 217–228. 11. A. V. DESAI, E. ELLIS, J. R. WHEATLEY: Fatal distraction: a case series of fatal fall-asleep road accidents
and their medical outcomes. Med. J. Aust., 178 (2003) 396–399.
12. M. KOSKENUOVO, M. PARTINEN, J. KAPRIO: Snoring as a risk factor for hypertension and angina
pectoris. Lancet, 1 (1985) 893–896.
13. J. F. MASA JIMENEZ, M. RUBIO GONZALEZ, L. J. FINDLEY: Sleepy drivers have a high frequency of
traffic accidents related to respiratory effort-related arousals. Arch. Bronconeumol., 39 (2003) 153–158.
14. N. CARTER, J. ULFBERG, B. NYSTROM: Sleep debt, sleepiness and accidents among males in the general
population and male professional drivers. Accid. Anal. Prev., 35 (2003) 613–617.
15. P. J. JENNUM, A. SJOL: Cognitive symptoms in persons with snoring and sleep apnea. An epidemiologic
study of 1.504 women and men aged 30–60 years. The Dan-MONICA II study. Ugeskr. Laeger, 157 (1995) 6252–6256.
RASCHE, J. P. MALIN: Accidents caused by sleepiness-prediction by
neurophysiologic/psychologic testing and simulated driving studies. Biomed. Tech. (Berlin),48 (2003) 55–61.
17. P. KÖVES: Az obstruktív alvási apnoe szindróma. Springer, 1998. 18. T. SHIOMI, A. T. ARITA, R. SASANABE: Falling asleep while driving and automobile accidents among
patients with obstructive sleep apnea-hypopnea syndrome. Psychiatry Clin. Neurosci., 56 (2002) 333–334.
19. J. ULFBERG, R. JONSSON, C. EDLING: Improvement of subjective work performance among obstructive
sleep apnea patients after treatment with continuous positive airway pressure. Psychiatry Clin. Neurosci.,53 (1999) 677–679.
20. C. SAUTER, S. ASENBAUM, R. POPOVIC: Excessive daytime sleepiness in patients suffering from
different levels of obstructive sleep apnoea syndrome. J. Sleep Research, 9 (2000) 293–301.
21. J. ULFBERG, N. CARTER, C. EDLING: Sleep-disordered breathing and occupational accidents. Scand. J. Work Environ. Health, 26 (2000) 237–242.
DIRECTORS’ AND OFFICERS’ LIABILITY WHAT’S AT STAKE IN DURA The Supreme Court’s return this Term to private securities litigation -- and its first consideration of the Private Securities Litigation Reform Act -- promises to bring needed clarity to the doctrine of loss causation. The proper standard for loss causation has been in court-acknowledged conflict for at least seven years.
IV Levetiracetam For Treatment of Cluster Headachein the ClinicJohn Claude Krusz PhD MD, Jane Cagle LVN, Dan Daniel RPHCASE 4: GF, a 41 year old businessman had reonset of cluster headache episodes, leftsided, 2 months prior to being seen. He was having 3-6 episodes per day, mostly at night. 4 years prior, he had first onset of cluster headaches lasting almost 6 weeks. IV INTRODUCTION: Levetir
 Z. SZAKÁCS & P. KÖVES: Obstructive sleep apnea syndrome
least 10 seconds. Hypopnea was identified as an at least 50-per-cent reduction in the amplitude of airflow for a minimum of 10 seconds and/or leading to a 4-per-cent reduction in SaO2, or precipitating physiological arousal (alpha-activity for 3 seconds at least). The apnea/hypopnea index (AHI) was calculated as the mean of cumulative apneic and hypopneic episodes occurring per hour of sleep.
Z. SZAKÁCS & P. KÖVES: Obstructive sleep apnea syndrome
least 10 seconds. Hypopnea was identified as an at least 50-per-cent reduction in the amplitude of airflow for a minimum of 10 seconds and/or leading to a 4-per-cent reduction in SaO2, or precipitating physiological arousal (alpha-activity for 3 seconds at least). The apnea/hypopnea index (AHI) was calculated as the mean of cumulative apneic and hypopneic episodes occurring per hour of sleep.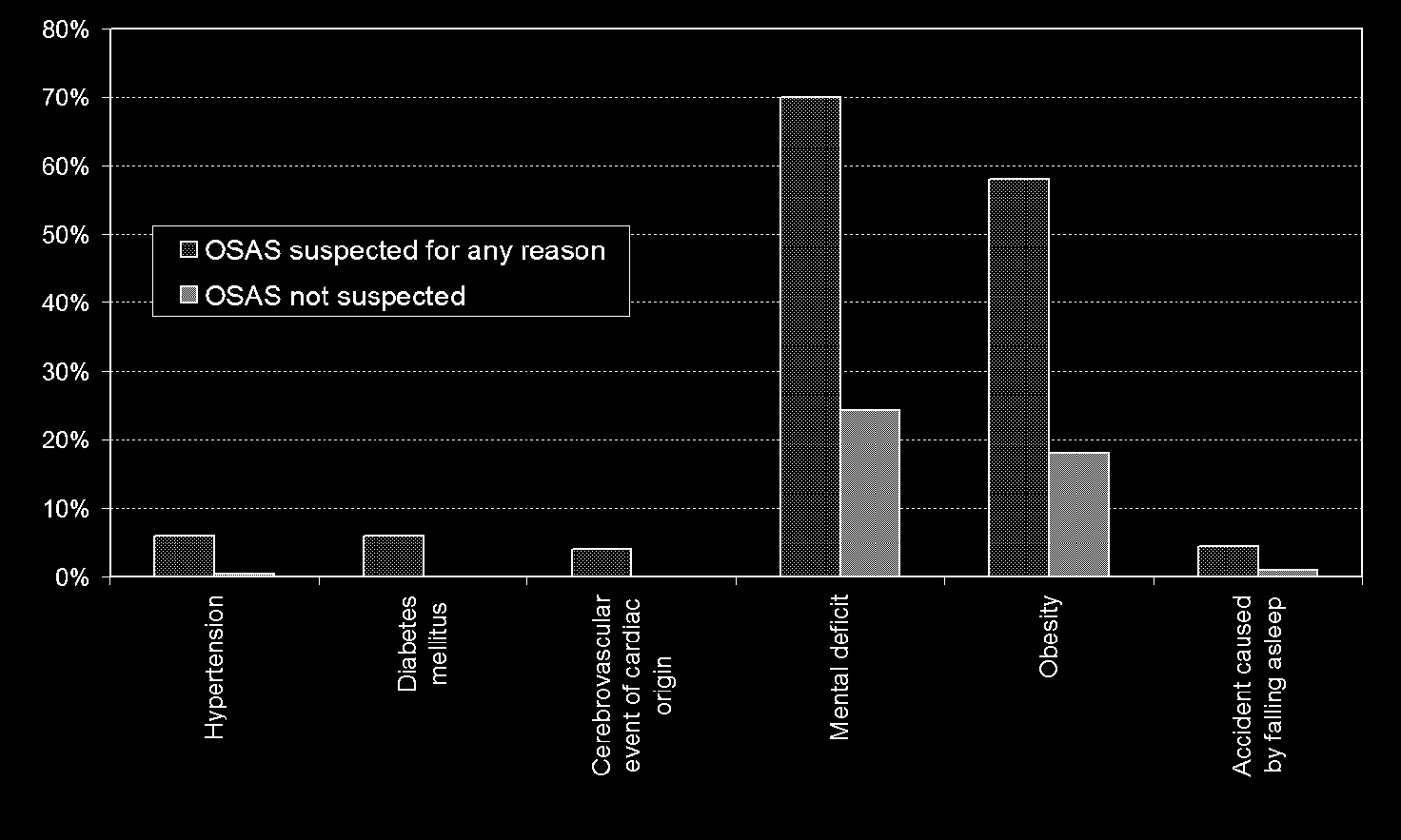 Z. SZAKÁCS & P. KÖVES: Obstructive sleep apnea syndrome
Results of screening
Z. SZAKÁCS & P. KÖVES: Obstructive sleep apnea syndrome
Results of screening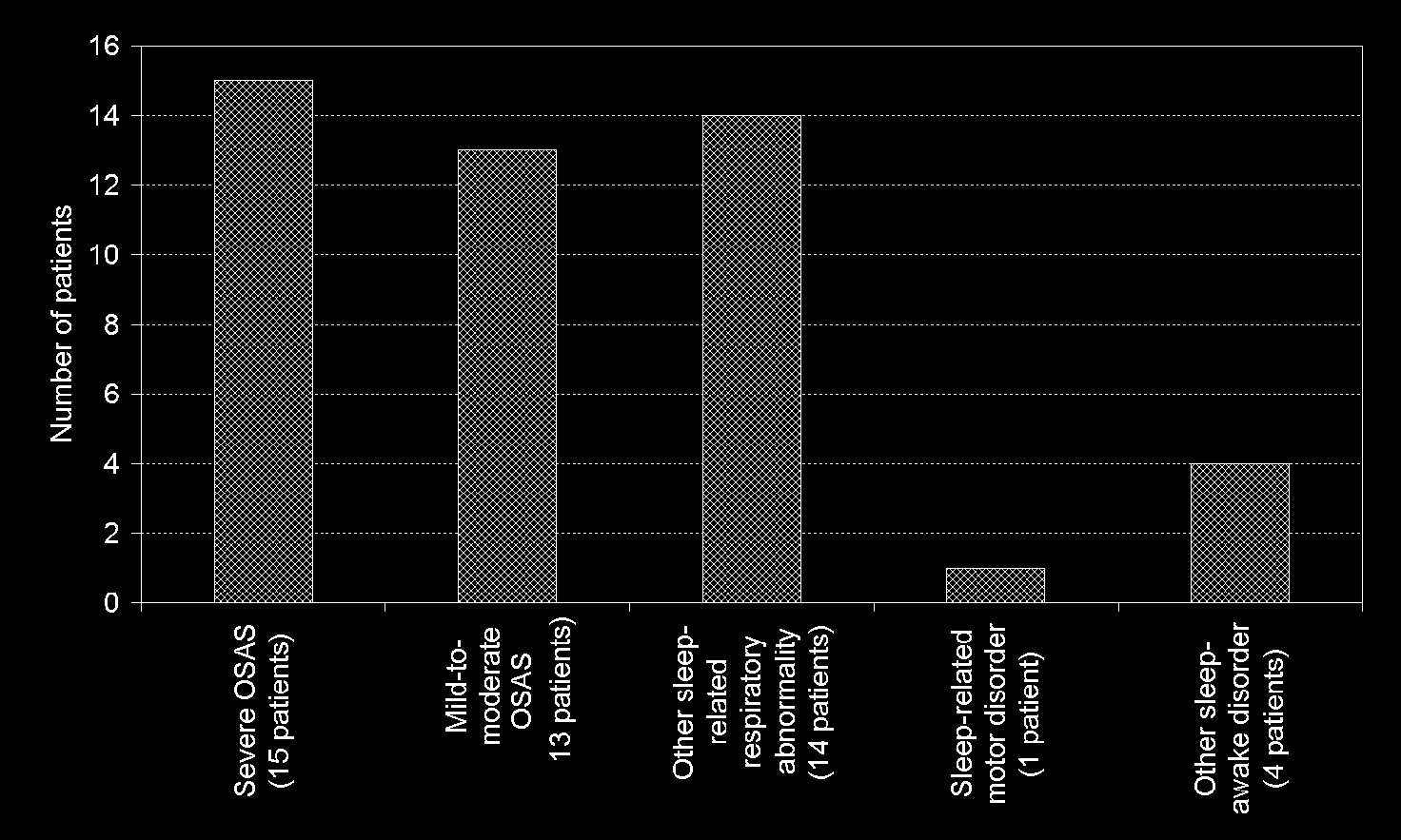 Z. SZAKÁCS & P. KÖVES: Obstructive sleep apnea syndrome
Among the 50 patients with suspected OSAS, 6% were hypertensive, 6% diabetic,
58% over-weight and 70% complained of mental deficit symptoms. A history of a cardiac-cerebrovascular event and of a road accident resulting from falling asleep were identified in 4–4% of these subjects (Figure 2).
Z. SZAKÁCS & P. KÖVES: Obstructive sleep apnea syndrome
Among the 50 patients with suspected OSAS, 6% were hypertensive, 6% diabetic,
58% over-weight and 70% complained of mental deficit symptoms. A history of a cardiac-cerebrovascular event and of a road accident resulting from falling asleep were identified in 4–4% of these subjects (Figure 2).