Respiratory Muscle Endurance Training in Chronic Obstructive Pulmonary Disease Impact on Exercise Capacity, Dyspnea, and Quality of Life THOMAS A. SCHERER, CHRISTINA M. SPENGLER, DOMINIK OWASSAPIAN, EDELBERT IMHOF, and URS BOUTELLIER
Department of Internal Medicine, Triemli Hospital, Zurich, and Department of Exercise Physiology, Federal Institute of Technologyand University of Zurich, Switzerland
Inspiratory muscle training may have beneficial effects in certain
which imitates most closely the load on the respiratory mus-
patients with chronic obstructive pulmonary disease (COPD). Be-
cles during exercise, was considered difficult to apply on a
cause of the lack of a home training device, normocapnic hyper-
large scale (14). In only one study was home-based training
pnea has rarely been used as a training mode for patients with
applied in conjunction with a comprehensive rehabilitation
COPD, and is generally considered unsuitable to large-scale appli- cation. To study the effects of hyperpnea training, we randomized
As compared with resistive breathing through a fixed ori-
30 patients with COPD and ventilatory limitation to respiratory
fice (0.5 cm) at a breathing rate of 15 breaths/min, or TL with
muscle training (RMT; n ϭ 15) with a new portable device or to
a threshold pressure of 30% of maximum inspiratory pressure
breathing exercises with an incentive spirometer (controls; n ϭ
) at a breathing rate of 15 breaths/min, normocapnic hy-
15). Both groups trained twice daily for 15 min for 5 d per week for
perpnea at a target minute ventilation ( E
8 wk. Training-induced changes were significantly greater in the
mal voluntary ventilation (MVV) generates the greatest work
RMT than in the control group for the following variables: respira-
of breathing (16). Prior work in subjects with COPD showed
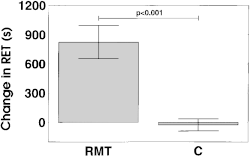
tory muscle endurance measured through sustained ventilation (ϩ825 Ϯ 170 s [mean Ϯ SEM] versus Ϫ27 Ϯ 61 s, p Ͻ 0.001), in-
that training with normocapnic hyperpnea improves respira-
spiratory muscle endurance measured through incremental in-
tory muscle endurance and exercise performance (5, 15). The
spiratory threshold loading (ϩ58 Ϯ 10 g versus ϩ21.7 Ϯ 9.5 g, p ϭ
effects of such training on dyspnea and quality of life, impor-
0.016), maximal expiratory pressure (ϩ20 Ϯ 7 cm H
tant outcome variables for patient compliance and well-being,
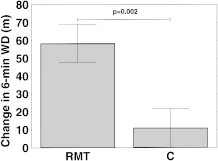
2O versus 0.009), 6-min walking distance ( 58 11 m versus 11 Ϯ 11 m, p ϭ 0.002), O
A recently developed training device allows respiratory
2.5 0.6 ml/kg/min versus
Ϫ0.3 Ϯ 0.9 ml/kg/min, p ϭ 0.015), and the SF-12 physical compo-
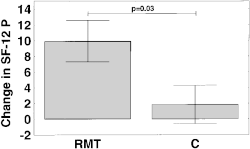
muscle training (RMT) with normocapnic hyperpnea at home. nent score (ϩ9.9 Ϯ 2.7 versus ϩ1.8 Ϯ 2.4, p ϭ 0.03). Changes in
Studies with healthy subjects using this device resulted in in-
dyspnea, maximal inspiratory pressure, treadmill endurance, and
creased cycling endurance (17) and decreased perceived respi-
the SF-12 mental component score did not differ significantly be-
ratory exertion during exercise (18). On the basis of these re-
tween the RMT and control groups. In conclusion, home-based
sults, we wanted to test the feasibility and effectiveness of
respiratory muscle endurance training with the new device used in
home training with this device in a randomized, controlled
this study is feasible and has beneficial effects in subjects with
study of subjects with COPD. The aim was not only to assess
COPD and ventilatory limitation.
the effects on respiratory muscle and exercise performance,but also to include the important variables of dyspnea and
Many patients with chronic obstructive pulmonary disease
(COPD) are limited in their physical activity by dyspnea. Lunghyperinflation, increased deadspace ventilation, and increased
energy consumption during hyperpnea lead to decreased ven-tilatory reserve and dyspnea on exertion (1, 2). Some subjects
The study protocol was approved by the ethics committee of the Tri-
with COPD show decreased maximal respiratory pressures (3,
4), which are indicative of respiratory muscle weakness and
Subjects
which may contribute to the perception of dyspnea.
Some studies have shown that the respiratory muscles can
Subjects were recruited from the outpatient clinic of the Pulmonary
be trained if an adequate training stimulus is applied, and that
Division of the Triemli Hospital. Consecutive patients were screenedby reviewing their charts and by interview. Those who met the inclu-
exercise performance (5, 6) and dyspnea (6, 7) may improve as
sion criteria, agreed to participate, and had signed the informed con-
a result of such training. In most studies inspiratory muscle
sent form were randomly assigned to an RMT group or a control
training has been done with resistive breathing or threshold
group, according to a computer-generated randomization table. Inclu-
loading (TL) (6–11). Few patients have been trained with nor-
sion criteria were chronic airflow obstruction (FEV Ͻ
mocapnic hyperpnea (5, 12, 13) because the complicated
equipment needed to prevent hypocapnia has usually required
after bronchodilatation with 200 g of albuterol inhaled from a pres-
a hospital facility or research laboratory, and has not been
surized metered-dose inhaler with a spacer), an age of 20 to 80 yr, and
available for home training. Therefore, this training mode,
a stable clinical condition for at least 1 mo. The patients’ physical ac-tivity had to be limited by pulmonary dyspnea only. In case of anypossibility that cardiac disease limited physical performance, patients
(Received in original form on December 7, 1999 and in revised form on May 4, 2000)
underwent cardiopulmonary exercise testing and echocardiography
Correspondence and requests for reprints should be addressed to Thomas A.
before inclusion in the study. Patients with dyspnea at rest, cardiac
Scherer, M.D., LungenZentrum Hirslanden, Witellikerstrasse 36, 8008 Zurich,
disease, poor compliance, drug or alcohol abuse, pregnancy or lacta-
Switzerland E-mail: thsche@swissonline.ch
tion, a requirement for supplemental oxygen, CO2 retention, or use of
Supported by grants from Astra Pharmaceutica, Dietikon, and Merck Sharpe and
any mechanical ventilatory support were excluded.
Dohme-Chibret, and Rhône-Poulenc Rorer.
Forty-nine patients were initially screened for the study. Ten pa-
Am J Respir Crit Care Med Vol 162. pp 1709–1714, 2000
tients refused to participate and five met one or more exclusion crite-
Internet address: www.atsjournals.org
ria. Thirty-four subjects were initially included. One patient assigned
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
to RMT withdrew during the initial testing and one control subject
ratory pressures (PImax and PEmax) measured at the mouth, and were
withdrew during Week 2 of the study. One patient in the RMT and
given a dyspnea questionnaire (baseline or transition dyspnea index),
one in the control group had to be excluded after traumatic hip and
6-min walking test, 20-min rest period, respiratory muscle endurance
rib fractures. Thirty subjects completed the study.
test (sustained ventilation), and health questionnaire, and underwent
Baseline characteristics of the study population are outlined in Ta-
measurement of peak oxygen consumption ( O
ble 1. The age range of the study population was 46 to 80 yr. No signif-
rest period, testing of inspiratory muscle endurance (TL), a third 20-
icant differences existed between the two study groups. During the
min rest period, and an endurance test on a treadmill.
study, subjects in the RMT group experienced 1.1 Ϯ 0.2 (mean Ϯ
Day 2. On Day 2 of the study the subjects had a 6-min walking test,
SEM) intercurrent illnesses, had 1.1 Ϯ 0.2 medication changes, and
20-min rest period, inspiratory muscle endurance test (TL), 20-min
had 1.3 Ϯ 0.5 missed training days per patient, versus 1.0 Ϯ 0.2 inter-
rest period, 6-min walking test, 20-min rest period, and second in-
current illnesses, 1.1 Ϯ 0.2 medication changes, and 0.7 Ϯ 0.3 missed
spiratory muscle endurance test (TL).
training days per patient, respectively, in the control group (no signif-icant differences existed between the RMT and control groups in
Pulmonary function tests were done according to American Tho-
racic Society criteria (19, 20), with measurement of slow VC, tidal vol-ume (VT), FVC, FEV1, peak expiratory flow (PEF), and 12-s MVV,
Study Protocol
with the Medical Graphics CPX/D System (Medical Graphics Corpo-ration, St. Paul, MN). Reference normal values were taken from the
All tests were performed in a standardized manner and sequence be-
European Community for Steel and Coal (21).
fore starting the training and 1 wk after its completion. Care was given
were measured from RV and TLC, respectively, with
that subjects were familiarized with the different tests and devices used.
a handheld device (Micro M.P.M.; Micro Medical Ltd., Rochester, UK)
Throughout the study period, subjects documented their training, their
that has a built-in small air leak to prevent pressure generation by glottis
pulmonary and other physical symptoms, physical activity, and any
closure. The highest pressure from among 10 measurements was re-
medication change in a diary, which, in addition to interviews of the
corded. Reference normal values were taken from Black and Hyatt (22).
subjects and evaluation of their training progress, served as a control
Endurance of the respiratory muscles was measured in two ways,
for compliance with the training program. The study was conducted in
a single-blind manner (i.e., subjects of both groups were told that theywere undergoing respiratory muscle training, and that two different de-
1. With the respiratory muscle endurance test to assess performance of
vices for this were being compared). The subjects in one group were
the inspiratory and expiratory muscles. This test was based on the
not informed about the device or training of the other group.
12-s MVV, which was performed three times. The highest MVV was
recorded. Respiratory muscle endurance was measured as sustainedventilation at 66% of each subject’s highest MVV. The time during
which subjects were able to sustain this target ventilation was re-
Day 1. On Day 1 of the study, subjects were given pulmonary func-
corded. If a subject surpassed 15 min of breathing at this level, the
tion tests (PFTs), had their 12-s MVV, maximal inspiratory and expi-
test was repeated on the following day at 75% of MVV. Subjectswere not coached and breathing was not paced. To assure nor-mocapnia, the training device (described subsequently), connectedto the metabolic cart (CPX/D system; Medical Graphics), was used. BASELINE CHARACTERISTICS OF THE GROUP ASSIGNED TO
ide pressure (PETCO ), and Sa (Minolta Pulsox 5; Minolta Switzer-
RESPIRATORY MUSCLE TRAINING AND CONTROL GROUPS
land, Dietikon, Switzerland) were measured continuously.
2. With the inspiratory muscle endurance test to assess performance
of the inspiratory muscles. This test was done with an inspiratory
TL device built according to the specifications of Nickerson and
Keens (23). The inspiratory threshold pressure was varied with
weights that were attached to a plunger, which closed the inspira-
tory valve. The initial threshold pressure was set to about 20% of
PImax. The weight was increased every 2 min by 50% of the initial
weight until the subject was unable to continue breathing. The
greatest weight the subject was able to sustain for at least 1 min was
taken as the measure for inspiratory muscle endurance. The test
was performed three times, and the greatest weight the subject en-
dured was recorded. Results were compared with normal reference
values established by Johnson and coworkers (24).
Exercise performance was tested with a 6-min walking test and a
treadmill endurance test. The 6-min walking test was performed in a
corridor of 90 m length. The subjects were instructed to cover as much
distance as possible during 6 min. They were not verbally coached,
but a person was walking about 1 m behind them. The test was re-
peated three times, and the longest distance walked was recorded.
Results were compared with normal reference values established by
Troosters and coworkers in healthy elderly subjects (25).
The endurance test on the treadmill was performed at a submaxi-
mal workload (see the subsequent discussion), and subjects were not
encouraged during this test. To determine the level of the submaximal
workload used in the test, peak power output and O
Definition of abbreviations: BDI ϭ Baseline Dyspnea Index; BMI ϭ body mass index;
MVV ϭ 12-s maximal voluntary ventilation; PE
sured with an incremental treadmill test by first gradually adjusting
maximal inspiratory pressure; PEF ϭ peak expiratory flow; RET ϭ respiratory muscle en-
the treadmill speed until the subject walked comfortably. The inclina-
durance measured as sustained ventilation; RMT ϭ respiratory muscle training; SF-12 P ϭ
tion of the treadmill was then increased by 2.5% in 2-min intervals un-
score on physical component of the SF-12 health questionnaire; SF-12 M ϭ score on
til the subject was exhausted. Normal reference values for O
mental component of the SF-12 questionnaire; TL ϭ inspiratory muscle endurance
were taken from Hansen and coworkers (26). To determine treadmill
measuring with threshold loading device; TM ϭ endurance on treadmill; E
endurance, the treadmill was set to 80% of the inclination and to
Scherer, Spengler, Owassapian, et al.: Respiratory Muscle Training
V 2peak speed was reduced by 20%. The test
cises. This was done by connecting the training device to the meta-
was terminated when subjects indicated that they were exhausted and
bolic cart and attaching a pulse oximeter to the subject’s finger. Dur-
unable to keep up with the speed of the treadmill. The time during
ing these weekly control sessions, breathing frequency was increased
which a subject was able to walk at the preset load was recorded as
reach a maximal training stimulus. Three subjects complained of dys-
Before training, dyspnea in daily activities was assessed with
pnea or dizziness during training. They were immediately called to the
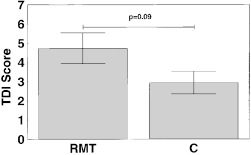
Mahler’s Baseline Dyspnea Index, and the change after training was
laboratory to monitor training instrument settings, SaO , and PET
assessed with Mahler’s Transition Dyspnea Index (TDI) (27, 28).
In the cases of two patients, settings had to be adjusted to correct for
Health-related quality of life was tested with the SF-12 health ques-
tionnaire (acute form), issued by the Medical Outcomes Trust (Bos-
The mean respiratory rate (RR) increased by 29% during the
ton, MA), which consists of a physical (SF-12 P) and a mental compo-
training period (p Ͻ 0.001; Week 1: 26.3 Ϯ 1.0 breaths/min; Week 2:
nent (SF-12 M) score. Because both questionnaires were originally
28.6 Ϯ 1.5 breaths/min; Week 3: 29.1 Ϯ 1.2 breaths/min; Week 4: 30.9 Ϯ
written in English, three persons fluent in English translated the ques-
1.5 breaths/min; Week 6: 32.6 Ϯ 1.8 breaths/min; Week 7: 33.5 Ϯ 2.1
tionnaires independently into German, and one bilingual person
breaths/min; and Week 8: 33.9 Ϯ 2.0 breaths/min). T
translated the German versions back into English. All translations
significantly during training (1.07 Ϯ 0.06 L at start of the training ver-
were compared, discussed, and adjusted to the most correct version.
sus 1.12 Ϯ 0.05 L at the end; p ϭ 0.50). Breathing Exercises in the Control Group
Respiratory muscle endurance training was done with a device that
Subjects in the control group were told that they were engaging in res-
we developed, consisting of tubing (I.D. ϭ 19 mm) that connects a re-
piratory muscle training with an incentive spirometer (COACH 2
breathing bag with a mouthpiece in a 90-degree angle. A sideport (of
Volumetric Incentive Spirometer; DHD Healthcare, Canastota, NY).
the same diameter as the tube) is inserted in the middle of this con-
This device was chosen for the sham training to give the subjects the
necting piece. This sideport contains a 6-mm hole that allows inspira-
impression that they were undergoing training. Because airflow resis-
tion from and expiration to fresh air, and also contains a valve. Sub-
tance through this device is minimal, and the RR during breathing ex-
jects fill and empty the rebreathing bag completely during inspiration
ercises was kept at about 6 to 8 breaths/min, we assumed that no train-
and expiration, while also inhaling additional fresh air through the
ing effect would result. The target inspiratory VT was set to 70% of
sideport during inspiration and breathing partly out through the side-
each subject’s VC. Subjects were instructed to breathe in slowly after
port during expiration. To assure a constant VT, the valve inserted in
a deep exhalation at a rate of 6 to 8 breaths/min, but their breathing
the sideport closes when subjects have emptied the bag during inspi-
was not paced. The exercises were performed twice daily for 15 min
ration. In our study the size of the bag was adjusted to 50 to 60% of
on 5 d per week for 8 wk. Splitting the exercises into 5-min sessions
the subject’s VC, and the breathing frequency chosen was such that
was allowed if the subject was unable to train for 15 min without inter-
V corresponded to 60% of MVV (monitored while the training de-
ruption. The subjects also had weekly control sessions of their breath-
vice was connected to the metabolic cart). Correct performance was
ing exercises without a change in VT or breathing rate.
checked by analyzing PETCO with the metabolic cart and Sa with the
Subjects in both the RMT and control groups who experienced
pulse oximeter. If PETCO deviated from normal baseline values during
acute breathing problems (e.g., due to an exacerbation of their
the 10- to 15-min trial run, VT was adjusted by changing the size of the
COPD) were allowed to stop training for a maximum of 14 d. These
rebreathing bag and breathing frequency was changed accordingly
subjects resumed their training from the same point at which they had
V at 60% of MVV. Values of training PETCO ranged from
stopped, in order to complete 40 training days.
33.1 Ϯ 1.1 mm Hg to 38.5 Ϯ 1.3 mm Hg. Hypocapnia during trainingwas corrected by increasing the size of the rebreathing bag, and hy-
Statistics
percapnia was corrected by decreasing the size of the bag. Hypoxemia
The results of the study are presented as mean Ϯ SEM. Because the
values were not normally distributed (normality of distribution was
While performing the breathing exercises, subjects wore a nose
tested with the Shapiro–Wille’s test), the nonparametric Mann–Whit-
clip to ensure breathing exclusively through the training device. The
ney U test was used to compare baseline characteristics and training-
exercises were performed twice daily for 15 min on 5 d per week for
related changes in the RMT and control groups, Wilcoxon’s matched
8 wk. Splitting the exercise into 5-min sessions was allowed if the sub-
pairs test was used to assess training-induced changes within a partic-
ject was unable to train for 15 min without interruption. Inspiration
ular group, and Friedman’s analysis of variance with Kendall’s con-
and expiration were paced by an electronic metronome (Seiko Digital
cordance was used to assess weekly changes over the course of the
Metronome; Seiko Corp., Tokyo, Japan).
training. A value of p Ͻ 0.05 was considered significant. The Statistica
Before the 8-wk training period and once every week during the
for Windows software program (Statsoft Inc., Tulsa, OK) was used for
, breathing rate, and VT were monitored in the
all calculations. To achieve a difference in change in respiratory mus-
pulmonary laboratory while subjects performed the breathing exer-
cle endurance of 20% with an SD of 50 s and a statistical power of80%, it was calculated that 12 to 15 patients had to be included in eachstudy group. The primary endpoint of the study was respiratory mus-
cle endurance; secondary endpoints were respiratory muscle strength,exercise performance, dyspnea, and health-related quality of life. TRAINING RELATED CHANGES IN THE GROUP ASSIGNED TO RESPIRATORY MUSCLE TRAINING AND IN THE CONTROL GROUP
Training-related changes in the RMT as compared with the
control group are shown in Table 2 and Figures 1 through 6. Figure 1. Change in respiratory
muscle endurance (RET), mea-sured as time of sustained ventila-
Definition of abbreviations: ⌬FEV1 ϭ change in forced expiratory volume in 1 s; ⌬FVC ϭ
change in FVC; ⌬PEmax ϭ change in maximal expiratory pressure; ⌬PImax ϭ change in
maximal inspiratory pressure; ⌬PEF ϭ change in peak expiratory flow; RMT ϭ respira-
tory muscle training; ⌬SF-12 M ϭ change in score on mental component of the SF-12
V 2peak ϭ change in maximal oxygen consumption.
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Figure 2. Change in inspiratory muscle endurance, measured with Figure 4. Change in score of the
Improvement in respiratory muscle endurance measured as
Keens and coworkers (12) found an increase from 74 to 109 L/
sustained ventilation (RMT group at 69 Ϯ 7% of MVV; con-
min (ϩ47%), and Levine and coworkers (13) found an in-
trol group at 70 Ϯ 5% of MVV) (Figure 1), and assessed with
crease from 56 to 79 L/min (ϩ41%) in MSVC. We are aware
incremental TL (Figure 2), was significantly greater in the
of only one study that evaluated home-based training (15).
RMT group. Likewise, change in PEmax (but not in PImax), in-
The investigators in this study achieved an increase from 34 to
crease in 6-min walking distance (Figure 3), O
physical (Figure 4) (but not the mental) component of the SF-12
Subjects in the present study also increased their exercise
health survey were significantly greater in the RMT than in
performance as a result of RMT. Their 6-min walking dis-
the control group. Both groups showed a decrease in dyspnea
in daily activities, but the difference was not significant (Fig-
changes were significantly larger in the RMT than in the con-
ure 5). Likewise, the change in treadmill endurance did not
trol group. The 58-m increase in 6-min walking distance in the
differ significantly between the two groups (Figure 6).
RMT group was large enough to be considered clinically rele-vant (29). Belman and Mittman (5) reported comparable re-
DISCUSSION
sults. A 6-wk period of training increased the 12-min walking
Our results in subjects with COPD and ventilatory limitation
distance from 1,058 m to 1,188 m (ϩ12%). Ries and Moser
show that home-based RMT with normocapnic hyperpnea im-
(15), who applied home-based respiratory muscle endurance
proved respiratory muscle endurance, exercise performance,
training in conjunction with pulmonary rehabilitation, ob-
health-related quality of life, and dyspnea in daily activities,
whereas pulmonary function did not change significantly.
min to 16.4 ml/kg/min (ϩ9%), and in 12-min walking distance,
Baseline characteristics, incidences of intercurrent illnesses,
from 943 m to 1,020 m (ϩ8%), which are also in the range of
and medication changes were comparable in the RMT and
our training-induced changes. Although the training-related
increase in treadmill endurance was considerably greater in
The inclusion criteria for the study were directed to chronic
the RMT group in our study, the changes did not differ signifi-
airflow limitation and limitation in physical activity by pulmo-
cantly between the two study groups. One reason for this in-
nary dyspnea. Respiratory muscle weakness and/or ventila-
significant difference may be that the individual improve-
tory limitation of physical activity were not prerequisites to
ments varied widely. The sample size was too small to reliably
study inclusion. Analysis of our data show, however, that ven-
exclude a difference in treadmill endurance, and a type II er-
tilatory limitation, reflected by high ventilation at
MVV of 85%), was clearly present. As compared with a
The increased exercise performance with RMT is impor-
healthy control population, our study subjects also had some
tant for patients with COPD, since it may help in their daily
weakness of their respiratory muscles, as expressed by their
activities. It is unclear, however, how this translates into an
improvement in dyspnea and quality of life, which are impor-
Imax, MVV, and TL. These findings probably had an ef-
fect on our results, and support the view that subjects with
tant parameters (30, 31). Without subjective benefits, patients
COPD, respiratory muscle weakness, and ventilatory limita-
will hardly be willing to engage in daily training of their respi-
ratory muscles. We therefore included the SF-12 Health Sur-
The hyperpnea training in our study was usually well toler-
vey and Mahler’s dyspnea indices in our study. The SF-12
ated. Only three patients called because they experienced ad-
Health Survey is a 12-item questionnaire that closely mirrors
verse effects, and their problems were readily solved.
the scores of the SF-36 short-form Health Survey (32), and
In RMT, the increase in respiratory muscle endurance,
which had proved to reflect health status in patients with
measured as sustained ventilation, was large (258%). Previous
chronic lung disease (33). The significant impact of RMT on
studies, using normocapnic hyperpnea as a training mode in
the physical component of the SF-12 health questionnaire is
subjects with COPD, had already demonstrated the beneficial
an important finding, because the effect of hyperpnea training
effects of this training mode on respiratory muscle endurance.
on quality of life has not yet been tested. It is already known
Using maximal sustained ventilatory capacity (MSVC) as a
that pulmonary rehabilitation with and without additional in-
measure of respiratory muscle endurance, Belman and Mitt-
spiratory muscle training can improve quality of life in pa-
man (5) reported an increase from 32 to 42 L/min (ϩ31%),
tients with COPD (34–36); however, the effect of RMT with-out additional intervention is unknown. Figure 3. Change in 6-min walking Figure 5. Change in Transition
durance training group; C ϭcontrol group.
Scherer, Spengler, Owassapian, et al.: Respiratory Muscle Training
(38–40). Currently, it is recommended that ventilatory muscletraining be considered within a pulmonary rehabilitation pro-
Figure 6. Change in treadmill
gram only for selected patients with decreased ventilatory
In summary, the results of the present study show that res-
piratory muscle endurance training with normocapnic hyper-pnea improves respiratory muscle and exercise performance,health-related quality of life, and dyspnea. The new portabletraining device used in the study makes home-based endur-ance training with normocapnic hyperpnea feasible, and al-
The TDI of 4.7 in our RMT group represents a distinct im-
provement in dyspnea. Lisboa and coworkers (6) reportedcomparable results after TL training at 30% of PImax. Their
References
subjects achieved significant increases in PImax (ϩ23 cm H2O;
ϩ34%) and 6-min walking distance (ϩ114 m; ϩ38%), and
1. Tobin MJ. Respiratory muscles in disease. Clin. Chest Med 1988;9:263–286. 2. Bauerle O, Chrusch CA, Younes M. Mechanisms by which COPD af-
these improvements were associated with a TDI of 3.8. In the
fects exercise tolerance. Am J Respir Crit Care Med 1998;157:57–68.
study by Harver and coworkers (7), subjects with COPD in-
3. Wijkstra PJ, van der Mark TW, Boezen M, van Altena R, Postma DS,
creased their PImax by 11 cm H2O (ϩ13%) after targeted in-
Koëter GH. Peak inspiratory mouth pressure in healthy subjects and
spiratory muscle training, which was associated with a TDI of
in patients with COPD. Chest 1995;107:652–656.
3.5. Lisboa and coworkers (6) reported that their subjects,
4. Rochester DF, Braun NT. Determinants of maximal inspiratory pres-
who trained with an inspiratory threshold load of 10% of their
sure in chronic obstructive pulmonary disease. Am Rev Respir Dis1985;132:42–47.
PImax, were able to increase their PImax by 12 cm H2O (ϩ19%),
5. Belman MJ, Mittman C. Ventilatory muscle training improves exercise
and this improvement was associated with a TDI of 1.7. Direct
capacity in chronic obstructive pulmonary disease patients. Am Rev
comparison of these studies done with different training modes
Respir Dis 1980;121:273–280.
is not possible. The optimal training mode in subjects with
6. Lisboa C, Villafranca C, Leiva A, Cruz E, Pertuzé J, Borzone G. Inspira-
tory muscle training in chronic airflow limitation: effect on exercise
The breathing exercises in our control group probably af-
performance. Eur Respir J 1997;10:537–542.
7. Harver A, Mahler DA, Daubenspeck A. Targeted inspiratory muscle
fected PImax (ϩ12 cm H2O; ϩ18%) and dyspnea (TDI ϭ 2.9).
training improves respiratory muscle function and reduces dyspnea in
Although we originally designed our study to have a control
patients with chronic obstructive pulmonary disease. Ann Intern Med
group undergoing sham training, subjects assigned to the con-
trol group experienced an improvement in their inspiratory
8. Larson JL, Kim JM, Sharp JT, Larson DA. Inspiratory muscle training
muscle performance. In some subjects who were eager to un-
with a pressure threshold breathing device in patients with chronic ob-
dergo training, this training effect was generated by the sub-
structive pulmonary disease. Am Rev Respir Dis 1988;138:689–696.
9. Lisboa C, Munoz V, Beroiza T, Leiva A, Cruz E. Inspiratory muscle
jects’ intention to continuously increase their training VT above
training in chronic airflow limitation: comparison of two different
the preset volume. Additionally, subjects who started inspira-
training loads with a threshold device. Eur Respir J 1994;7:1266–1274.
tion at a level well above their FRC generated some load on
10. Pardy RL, Rivington RN, Despas PJ, Macklem PT. Inspiratory muscle
their inspiratory muscles at the end of inspiration. We assume
training compared with physiotherapy in patients with chronic airflow
that the improvement in these subjects’ dyspnea resulted from
limitation. Am Rev Respir Dis 1981;123:421–425.
their increased inspiratory muscle performance, as reflected
11. Wanke T, Formanek D, Lahrmann H, Brath H, Wild M, Wagner CZH.
Effects of combined inspiratory muscle and cycle ergometer training
by the increase in their PImax and inspiratory muscle endur-
on exercise performance in patients with COPD. Eur Respir J 1994;
ance. Although it can be argued that these changes were a pla-
cebo effect or based purely on motivation, the fact that PImax
12. Keens TG, Krastins IRB, Wannamaker EM, Levison H, Crozier DN,
Bryan AC. Ventilatory muscle endurance training in normal subjects
volving unaffected expiratory muscles) improved suggests that
and patients with cystic fibrosis. Am Rev Respir Dis 1977;116:853–860.
a mild training effect occurred. The increase in P
13. Levine S, Weiser P, Gillen J. Evaluation of a ventilatory muscle endur-
ance training program in the rehabilitation of patients with chronic
control group may have been at least partly responsible for the
obstructive pulmonary disease. Am Rev Respir Dis 1986;133:400–406.
lack of difference in the training-induced change in PImax be-
14. Gosselink R, Decramer M. Inspiratory muscle training: where are we?
Eur Respir J 1994;7:2103–2105.
15. Ries AL, Moser KM. Comparison of normocapnic hyperventilation and
greater in the RMT than in the control group. This was proba-
walking exercise training at home in pulmonary rehabilitation. Chest
bly caused by the load on the expiratory muscles induced by
16. Belman MJ, Botnick WC, Nathan SD, Chon KH. Ventilatory load char-
the hyperpnea training. Suzuki and coworkers (37) reported
acteristics during ventilatory muscle training. Am J Respir Crit Care
that expiratory muscle training in healthy subjects could im-
prove expiratory muscle strength and decrease E
17. Spengler CM, Roos M, Laube SM, Boutellier U. Decreased exercise
sensation of respiratory effort during exercise. It is conceiv-
blood lactate concentrations after respiratory endurance training in
able that the increase in expiratory muscle strength in our
humans. Eur J Appl Physiol 1999;79:299–305.
RMT group contributed to the decrease in their dyspnea. Fur-
18. Spengler CM, Lenzin C, Stüssi C, Markov G, Boutellier U. Decreased
perceived respiratory exertion during exercise after respiratory endur-
ther studies are needed to clarify this issue.
ance training [abstract]. Am J Respir Crit Care Med 1998;157:A782.
RMT with normocapnic hyperpnea requires personal effort
19. American Thoracic Society. Standardization of spirometry—1994 up-
and good motivation. Of the 49 persons screened for our
date. Am J Respir Crit Care Med 1995;152:1107–1136.
study, 10 refused to participate, mainly because of lack of mo-
20. American Thoracic Society. Lung function testing: selection of reference
tivation. This shows that not every patient is a good candidate
values and interpretative strategies. Am J Respir Crit Care Med 1991;
for this kind of treatment. Furthermore, it remains to be clari-
21. European Community for Steel and Coal. Standardized lung function
fied whether the addition of RMT to a pulmonary rehabilita-
testing. Eur Respir J 1993;6(Suppl 16):25–27.
tion program is worthwhile, and which patients in particular
22. Black LF, Hyatt RE. Maximal respiratory pressures, normal values and
will benefit from it. Results of published trials are equivocal
relationship to age and sex. Am Rev Respir Dis 1969;99:696–702.
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
23. Nickerson BG, Keens TG. Measuring ventilatory muscle endurance in
related quality of life in chronic lung disease. J Gen Intern Med 1994;
humans as sustainable inspiratory pressure. J Appl Physiol 1982;52:
34. Dekhuijzen PNR, Folgering HTM, van Herwaarden CLA. Target-flow
24. Johnson PH, Cowley AJ, Kinnear WJM. Incremental threshold loading:
inspiratory muscle training during pulmonary rehabilitation in pa-
a standard protocol and establishment of a reference range in naive
tients with COPD. Chest 1991;99:128–133.
normal subjects. Eur Respir J 1997;10:2868–2871.
35. Wijkstra PJ, VanAltena R, Kraan J, Otten V, Postma DS, Koëter GH.
25. Troosters T, Gosseling R, Decramer M. Six minute walking distance in
Quality of life in patients with chronic obstructive pulmonary disease
healthy elderly subjects. Eur Respir J 1999;14:270–274.
improves after rehabilitation at home. Eur Respir J 1994;7:269–273.
26. Hansen JE, Sue DY, Wasserman K. Predicted values for clinical exercise
36. Wijkstra PJ, TenVergert EM, VanAltena R, Otten V, Kraan J, Postma
testing. Am Rev Respir Dis 1984;129:S49–S55.
DS, Koëter GH. Long term benefits of rehabilitation at home on qual-
27. Mahler DA, Wells CK. Evaluation of clinical methods for rating dysp-
ity of life and exercise tolerance in patients with chronic obstructive
nea. Chest 1988;93:580–586.
pulmonary disease. Thorax 1995;50:824–828.
28. Mahler DA, Tomlinson D, Olmstead EM, Tosteson AN, O’Connor GT.
37. Suzuki S, Sato M, Okubo T. Expiratory muscle training and sensation of
Changes in dyspnea, health status, and lung function in chronic air-
respiratory effort during exercise in normal subjects. Thorax 1995;50:
ways disease. Am J Respir Crit Care Med 1995;151:61–65.
29. Redelmeier DA, Bayoumi AM, Goldstein RS, Guyatt GH. Interpreting
38. Lacasse Y, Guyatt GH, Goldstein RS. The components of a respiratory
small differences in functional status: the six-minute walk test in
rehabilitation program: a systematic overview. Chest 1997;111:1077–
chronic lung disease patients. Am J Respir Crit Care Med 1997;155:
39. Tiep BL. Disease management of COPD with pulmonary rehabilitation.
30. Curtis JR, Martin DP, Martin TR. Patient-assessed health outcomes in
chronic lung disease. Am J Respir Crit Care Med 1997;156:1032–1039.
40. Larson JL, Covey MK, Wirtz SE, Berry JK, Alex CG, Langbein E, Ed-
31. Testa MA, Simonson DC. Assessment of quality-of-life outcomes. N
wards L. Cycle ergometer and inspiratory muscle training in chronic
Engl J Med 1996;334:835–840.
obstructive pulmonary disease. Am J Respir Crit Care Med 1999;160:
32. Jenkinson C, Layte R, Jenkinson D, Lawrence K, Petersen S, Paice C,
Stradling J. A shorter form health survey: can the SF-12 replicate re-
41. American College of Chest Physicians/American Association of Cardio-
sults from the SF-36 in longitudinal studies? J Public Health Med
vascular and Pulmonary Rehabilitation. Pulmonary Rehabilitation
Guidelines Panel. Pulmonary rehabilitation: joint ACCP/AACVPR
33. Viramontes JL, O’Brien B. Relationship between symptoms and health-
evidence-based guidelines. Chest 1997;112:1363–1396.
Zagazig University Faculty of Science Department of Geology AN INTEGRATED STUDY OF POTENTIAL AND SEISMIC METHODS ON SOUTH SITRA AREA, WESTERN DESERT, EGYPT. To the Department of Geology, Faculty of Science, Supervisors Late Prof. Dr. M. A. Shabaan Prof. Dr. Ali Ali El-Khadragy Prof. Dr. Salah Shebl Saleh Dr. Mohamed Housein Saad Zagazig University Facu
FLUID COMPATIBILITY CHART for metal threaded fittings sealed with Loctite ® Sealants LIQUIDS, SOLUTIONS & SUSPENSIONS Loctite product numbers in red are worldwide or application-specific products(This is a list of chemical stability only. It does not constitute approval for use in the processing of food, drugs, cosmetics, pharmaceuticals, andingestible chemicals.) Loctite® sealants
 Scherer, Spengler, Owassapian, et al.: Respiratory Muscle Training
V 2peak speed was reduced by 20%. The test
cises. This was done by connecting the training device to the meta-
was terminated when subjects indicated that they were exhausted and
bolic cart and attaching a pulse oximeter to the subject’s finger. Dur-
unable to keep up with the speed of the treadmill. The time during
ing these weekly control sessions, breathing frequency was increased
which a subject was able to walk at the preset load was recorded as
reach a maximal training stimulus. Three subjects complained of dys-
Before training, dyspnea in daily activities was assessed with
pnea or dizziness during training. They were immediately called to the
Mahler’s Baseline Dyspnea Index, and the change after training was
laboratory to monitor training instrument settings, SaO , and PET
assessed with Mahler’s Transition Dyspnea Index (TDI) (27, 28).
Scherer, Spengler, Owassapian, et al.: Respiratory Muscle Training
V 2peak speed was reduced by 20%. The test
cises. This was done by connecting the training device to the meta-
was terminated when subjects indicated that they were exhausted and
bolic cart and attaching a pulse oximeter to the subject’s finger. Dur-
unable to keep up with the speed of the treadmill. The time during
ing these weekly control sessions, breathing frequency was increased
which a subject was able to walk at the preset load was recorded as
reach a maximal training stimulus. Three subjects complained of dys-
Before training, dyspnea in daily activities was assessed with
pnea or dizziness during training. They were immediately called to the
Mahler’s Baseline Dyspnea Index, and the change after training was
laboratory to monitor training instrument settings, SaO , and PET
assessed with Mahler’s Transition Dyspnea Index (TDI) (27, 28).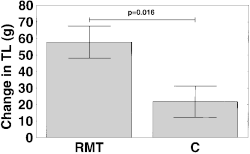
 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Figure 2. Change in inspiratory
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Figure 2. Change in inspiratory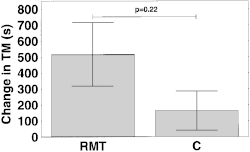 Scherer, Spengler, Owassapian, et al.: Respiratory Muscle Training
(38–40). Currently, it is recommended that ventilatory muscletraining be considered within a pulmonary rehabilitation pro-
Figure 6. Change in treadmill
Scherer, Spengler, Owassapian, et al.: Respiratory Muscle Training
(38–40). Currently, it is recommended that ventilatory muscletraining be considered within a pulmonary rehabilitation pro-
Figure 6. Change in treadmill