B R I T I S H J O U R N A L O F P S YC H I AT RY ( 2 0 0 4 ) , 1 8 5 , 3 1 ^ 3 6
fog?’). After a telephone screening, poten-
tially suitable individuals were seen for aninitial clinical evaluation. For inclusion in
the study, individuals had to have takenno psychotropic medication for a period
oxidase inhibitors or investigational drugs). Applicants were not eligible if they hadpreviously undergone an adequate fluox-etine trial, defined as a minimum of 10 mgdaily for 4 weeks, or if they reported fluox-etine intolerance or hypersensitivity.
Depersonalisation disorder is characterised
ten informed consent was obtained after a
full explanation of the study by the princi-
order is diagnosed when depersonalisation
is persistent or recurrent, causes marked
distress or impairment, and is not part of
another psychiatric or medical condition.
The illness is often chronic and debilitating,
bipolar disorder or organic mental disorder
were excluded from the study, as were indi-
viduals with current substance use disorder
or eating disorder. Lifetime Axis I disorders
were assessed using the Structured Clinical
(First et al, 1995), and Axis II personality
disorders were assessed with the Structured
et al, 1990; Fichtner et al, 1992; Ratliff &
orders (Pfohl et al, 1995). Participants were
allowed to enter the trial if they had been
masked, placebo-controlled trial. We pre-
psychotherapy or were receiving specialised
treatment such as cognitive–behavioural
therapy and hypnosis were excluded. Indi-
viduals with acute or unstable medical ill-
nesses, as well as those with a history of
seizure disorder or major head trauma,were also excluded. All participants had a
normal baseline routine laboratory evalua-
tion with negative urine toxicology screen-
People eligible for the study were adults
required to use an effective birth control
aged 18–65 years, who met DSM–IV diag-
nostic criteria for current depersonalisation
disorder by semi-structured clinical inter-
view and by the Structured Clinical Inter-
ised, parallel, flexible-dosage comparison
of fluoxetine v. placebo for the treatment
and postulate persistent depersonalisation,
of depersonalisation disorder. After a 2-
with intact reality testing, not occurring
exclusively in the context of another diag-
identical-appearing fluoxetine or placebo
Association, 1994). Participants were self-
capsules. Participants were assigned to the
referred by responding to newspaper adver-
fluoxetine or placebo group by the institu-
tisements for research (‘do you frequently
tion’s pharmacy on the basis of a standard
investigators. Fluoxetine dosage was 10 mg
in the past week only; in this context it
other controlling for depression and anxiety
per day for the first week, flexibly increased
has been shown to be sensitive to treatment
to 20 mg, 40 mg or 60 mg per day over the
change (Ellason & Ross, 1997; Lubin et al,
baseline scores were used as the only co-
following 3 weeks, according to tolerabil-
factor analysis of the DES in people with
additional covariates in order to control
the previously anecdotally reported efficacy
for baseline and treatment effects in anxi-
of higher dosages (Hollander et al, 1990),
three factors – absorption, amnesia and de-
ety, depression and social anxiety, using
not required if not tolerated. No concomi-
as well as change scores in these variables
tant medication was allowed for the entire
between baseline and week 10. Obsessive–
on the particular factor analysis (mean of
Table 3). Specifically for the CGI–I ana-
lyses, the baseline CGI–S score was used
adjusted the medication dose. Subsequently,
The Depersonalization Severity Scale (DSS;
as the covariate, and for the four people
the independent evaluator (O.G.), to whom
Simeon et al, 2001) is a six-item, clinician-
participants had been requested to report
visit, a CGI–I score of 4 was assumed. For
all symptoms accurately but without refer-
experiences rated 0–3, applied to the past
week, which takes into account both symp-
0.80 in detecting group differences with a
two-tailed test at the 0.5 level of signifi-
cance, the effect size (difference between
convergent and divergent validity, and to
A categorical analysis of responders v.
come measures were used, in order to give
test, defined as a CGI–I score of 2 or 1,
were clinician-administered at each visit. Depression was measured using the 17-item
measures. Chi-squared tests were also used
The Clinical Global Impression scale (CGI;
acteristics of the two groups where appro-
Guy, 1976) is a standard clinician-rated,
Rating Scale for Anxiety (HRSA; Hamilton,
response in relation to the presence of Axis
was applied at the initial visit, and the
I or Axis II disorders. For all 262 w2 tests
during all subsequent visits, specifically to
social anxiety and consequent avoidance.
measured using the Yale–Brown Obsessive
al, 1989), a ten-item scale that measures
Bernstein-Carlson & Putnam, 1993) is by
far the most widely applied measure of dis-
record of total number of panic attacks. In
research studies to date. It is a 28-item
addition to these scales, CGI–I scores were
self-report questionnaire of dissociative
applied to all existent comorbid disorders
to measure treatment change in each.
Fifty-four people entered the placebo run-in
period, of whom four were not randomised:
has been shown to have good test–retest
reliability (intraclass correlation coefficient
sequent visit, one experienced a complete
formed, with last observation carried for-
resolution of depersonalisation symptoms,
(Cronbach’s a¼0.95) and strong conver-
and one experienced severe adverse effects
gent, discriminant and criterion validity.
complete the trial. For each of the three
on placebo. Of the 50 participants random-
ised, 25 to fluoxetine and 25 to placebo,
three-quarters (37) completed the trial, 16
patients are asked to rate their experience
F LUOX E T I N E T R E AT M E N T O F D E P E R S ON A L I S AT I ON
was a trend toward more people withdepressive disorders in the fluoxetine groupand more people with anxiety disorders in
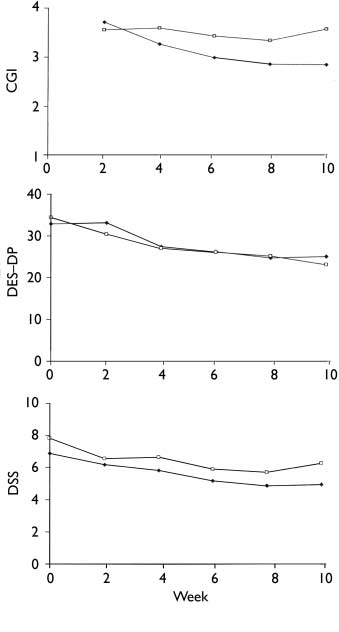
fluoxetine was not superior to placebo in
treating depersonalisation, with the excep-
tion of a statistically significant improve-
although statistically greater than the pla-cebo mean improvement of 3.6. Bi-weekly
categorical analysis of responder status re-
(n¼6) and a 20% response rate on placebo
(n¼5) (w2¼0.12, d.f.¼1, P¼0.73).
two groups as a whole. However, if the par-ticipants who had a diagnosis of depressive
(Table 2), those taking fluoxetine consis-
tently tended to have better responses than
CGI–I scores of 2 or 1 for the particular dis-
order: 50% v. 0% for major depression,75% v. 25% for dysthymia, 50% v. 40%
for generalised anxiety disorder, 100% v.
25% for obsessive–compulsive disorder,50% v. 40% for panic disorder and 33%
(w2¼2.60, d.f.¼1, P¼0.11). The mean daily
tion (CGI–I 1). Withdrawals from the pla-
depersonalisation disorder CGI–I score in
fluoxetine and 46 mg for placebo (t¼0.45,
for as follows: two persons before week 2,
only primary outcome variable to show dif-
to covarying for anxiety and depression.
For the fluoxetine group, end-point CGI–I
to seek private treatment and one with wor-
not significantly differ according to the pre-
sening anxiety; three persons before week
4, one to attempt impregnation (CGI–I 5),
istics of the 50 participants with DSM–IV
(CGI–I) in comorbid depressive disorders
one to seek private treatment (CGI–I 4)
(w2¼5.07, d.f.¼4, P¼0.28). However, end-
and one discontinued by the investigators
point CGI–I for depersonalisation disorder
for worsening depression (CGI–I 3); two
did marginally differ according to the pre-
marised in Table 2. It can be seen that the
tion) before week 8 (CGI–I 2 and 4); and
(w2¼5.76, d.f.¼2, P¼0.06). In effect, of
(48% fluoxetine, 20% placebo) and de-creased sexual arousal (24% fluoxetine,4% placebo). Only one person from the
fluoxetine group discontinued the trial pre-
maturely because of adverse effects, in this
case heightened anxiety. Therefore, to ourknowledge, the greater withdrawal
the medication arm was not due to adverse
possible efficacy suggested by earlier anec-
dotal data. Previous reports had found that
improvement in depersonalisation was clo-
sely related to the presence of other symp-toms responsive to serotonin reuptake
spective treatment reviews in depersonalisa-
efficacy for serotonin reuptake inhibitor
in both treatment groups, which was clini-
cally not noteworthy and statistically no
CGI–I score in the fluoxetine group, before
effects, was also not clinically significant,
approximately 3, i.e. minimal change.
Indeed, a number of the participants whoexperienced some improvement
tine expressed this effect in words, stating
fluoxetine, 4% placebo), muscle stiffness
to take less notice or be less bothered by
responders were all depersonalisation dis-
them. The study finding of slight improve-
40% placebo), excitation or hyperactivity
whose anxiety disorder did not respond to
fluoxetine, only one was a depersonalisa-
responder status did not significantly differ
in the presence or absence of personality
placebo), stomach ache (12% both groups),
disorder (w2¼0.00, d.f.¼1, P¼1.00).
It is possible that some alleviation of co-
morbid anxiety and depression contributed
to an overall more tolerable affective state,
Side-effects occurring at a frequency of at
which led participants to experience their
least 10% in at least one of the two study
depersonalisation as less troubling although
fluoxetine, 24% placebo), decreased libido
essentially unchanged. Indeed, a mediating
F LUOX E T I N E T R E AT M E N T O F D E P E R S ON A L I S AT I ON
effect of comorbid anxiety and depression
is suggested by the loss of statistically
ised depersonalisation as a universal pre-
formed functional response of the brain to
covaried for baseline and change in anxiety
and depression, as well as by the greaterimprovement
improvement in anxiety disorders in those
fluoxetine, compared with non-responders.
Strengths of the study include the fluoxetine
well-validated dissociation measures, both
for decades, and it would be fair to say that
clinician-rated and self-reported; the use
relationship of depersonalisation to phobic
anxiety (Roth, 1959), depression (Sedman,
stringent selection criteria for the partici-
pants with primary DSM–IV depersonalisa-
arm, and the medium size of the sample.
and anxiety disorders (Baker et al, 2003). An alternative view, however, is thatextreme emotional states such as severe
depression or anxiety are one type of ‘trau-
Our study suggests that first-line use of
matic stress’, among many others, that may
serotonin reuptake inhibitors for the treat-
ment of depersonalisation disorder is not
with an underlying vulnerability; in some
indicated, except possibly in selected indi-
viduals with troublesome anxiety or depres-
chronic and autonomous of the precipitat-
sion; in such individuals, improved affective
ing stressor (Simeon et al, 2003). The lack
of responsiveness of depersonalisation to
tolerance of their dissociative symptoms.
fluoxetine supports the latter concept, that
depersonalisation disorder is a distinct dis-
study are important in light of the absence
sociative disorder. Indeed, as long ago as
depersonalisation, and the common clinicalpractice of the past decade of using seroto-
nin reuptake inhibitors on the basis ofpromising early anecdotal reports and the
frequent presence of comorbid anxietyand depression. In the future, investigating
other classes of medications that may have
N O N - M E D I C I N A L I N G R E D I E N T SI N T E R A C T I O N S & C O N T R A D I C T I O N SP H A R M A C E U T I C A L C O M M E N T A R Y Vitamin B12 Cyanocobalamin Ingredients (alphabetical) Medicinal: CyanocobalaminNon-medicinal: Cellulose, magnesium stearate vegetable grade (lubricant) Allergens Supplemental vitamin B12 is used primarily to ensure sufficient cyanoco
 F LUOX E T I N E T R E AT M E N T O F D E P E R S ON A L I S AT I ON
effect of comorbid anxiety and depression
is suggested by the loss of statistically
ised depersonalisation as a universal pre-
formed functional response of the brain to
covaried for baseline and change in anxiety
and depression, as well as by the greaterimprovement
improvement in anxiety disorders in those
fluoxetine, compared with non-responders.
F LUOX E T I N E T R E AT M E N T O F D E P E R S ON A L I S AT I ON
effect of comorbid anxiety and depression
is suggested by the loss of statistically
ised depersonalisation as a universal pre-
formed functional response of the brain to
covaried for baseline and change in anxiety
and depression, as well as by the greaterimprovement
improvement in anxiety disorders in those
fluoxetine, compared with non-responders.