Microsoft powerpoint - diabetes medications april 2011.ppt
“Making Clinical Sense of Diabetes Types of Diabetes Medications”
Type 1 DM = Beta Cell Destruction, absolute insulin deficiency
Type 2 DM = Ranges from predominantly insulin
resistance with relative insulin deficiency to
predominantly insulin deficiency with insulin
Gestational DM (GDM) = glucose intolerance with
Pre-Diabetes = Impaired Fasting Glucose (IFG) or Impaired Glucose Tolerance (IGT)
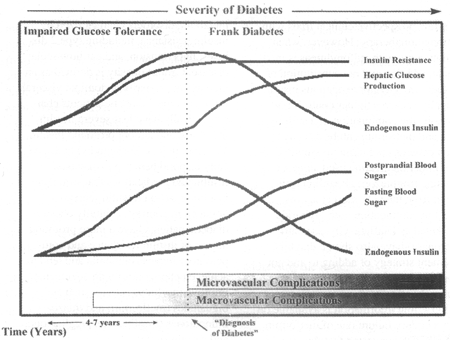
Pathophysiology Beta Cell Function & Glucagon
Insulin Deficiency + Insulin Resistance =
Progressive Beta cell decline = inadequate insulin
Hyperglycemia Type 2 DM, Gestational DM, Pre-
Absolute Deficiency of Insulin = Hyperglycemia
Glucagon is not suppressed during the post prandial
Hepatic glucose production is increased during the fasting period
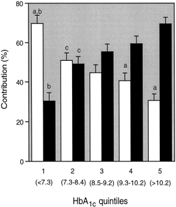
Relative contributions of postprandial (□) and
fasting (▪) hyperglycemia (%) to the overall diurnal hyperglycemia over quintiles of HbA1c
Optimal Diabetes Medication Glycemic Targets Management
Address patient concerns, i.e. hypo, weight gain, side
Oral Medications Question #1
• Drugs in the sulfoynlurea class are the drug of
Pancreas – stimulate insulin production
choice for newly diagnosed Type 2 diabetes
Liver – decrease hepatic glucose production
Intestines/gut – decrease absorption of CHO; gut
Sulfonylureas Sulfonylureas
Efficacy: Reduce A1C 1-2%, decrease FPG 60
Work best in first 5-10 years of diabetes
Meglinitides Meglinitides (continued)
Take 0-15 min before meals and large snacks
Efficacy: Reduce A1C 1-2%, Decrease FGB, PPG
Question #2 Question #3
Which of the following is an important counseling
Metformin is one of the best choices to target post
c. May cause GI upsetd. If you skip a meal, skip Prandin
Biguanides Biguanides (continued)
Action: Decrease hepatic gluconeogenesis and
Efficacy: Reduce A1C 1-2%, decrease FPG 60-70
mg/dl, weight loss, may decrease cholesterol
Contraindicated if serum Cr > 1.4 mg/dl women,
Thiazolidenediones (TZDs) TZDs (continued) Alpha-Glucosidase Inhibitors AGIs (continued)
Action: Delay digestion and absorption of CHO
Inhibit intestinal enzyme →slow breakdown of complex
Decrease FBG (20-30 mg/dl) and PPG (40-50 mg/dl)
DPP-4 Inhibitors DPP-4 Inhibitors (continued)
Ingestion of food→release of incretin hormones
GLP-1 and GIP→Beta & Alpha cell stimulation
In DM, DPP-4 enzyme breaks down GLP-1 & GIP,
so that the beta/alpha cells have decreased
These inhibit the DDP-4 enzyme→prolongs life of GLP-1
Combination Meds Incretin Mimetics
Action: increase insulin secretion, B-cell
growth/replication, slows gastric emptying, may
• Actosplus Met (pioglitazone/metformin)
decrease food intake, suppresses glucagon secretion
• Duetact (pioglitazone/glimepiride) • Janumet (sitagliptin/metformin)
• Avandaryl (rosiglitazone/glimepiride) • Kombiglyze XR (metformin/saxagliptin)
Incretin Mimetics (continued) Question #4
Which medication(s) do not have the side effect of
Risks: nausea, not with CrCL< 30mg/dl, not with
Amylinomimetc Amylinomimetic (continued)
Action: Hormone amylin co-secreted by beta cells in
Dose T1DM 15 mcg→60mcg 4 step titration
Dose T2 DM 60mcg→120 mcg 2 step titration
Deficiencies relative to beta cell function
Reduces food intake, appetite suppression
Dopamine Agonist Bile Acid Sequestrant
Used with diet & exercise in Type 2 DM
GI side effects (constipation, dyspepsia, nausea)
Insulin Therapy Insulin Duration Insulin Insulin: Basal/Bolus Regimen
NPH, detemir (Levemir), glargine (Lantus)
Detemir & glargine more physiologic for basal
Basal/Bolus Regimen Insulin
Bolus insulin targets meals/snacks and post prandial glucose
• Add rapid insulin to next largest meal
Insulin Case Study #1
S.B. is a 42 yo AAF, 5 year hx Type 2 DM. PMH
includes HTN, Ht 61 inches, wt 163 #; labs A1C
10.2%, HDL 55 mg/dl, LDL 83 mg/dl, TG 111, TC
167, SCr 0.9. Meds: lisinopril, metformin 1000 mg
bid, glyburide 5 mg bid, asa 81 mg qd.
Q: Which of the following is the most effective
approach to improve SBs glycemic control?
Case Study #1 Case Study #2
T.L. is a 72 yo Caucasian male with 15 year hx DMT2. Meds: glipizide 10 mg bid, precose 25 mg
tid ac, simvastatin. FBG 113-190, tests BG only in the am. BP 143/63, 6 ft 1 in, 220 #, SCr 1.7, HDL
26, LDL 79, TG 182, TC 120. A1C 8.2%. He reports he often forgets to take the precose.
Q: Which of the following is the most effective approach to improve TLs glycemic control?
Case Study #2 Case Study #3
J.R. is a 40 yo AAM, 20 yr hx DMT2. Patient currently taking Lantus 20 units HS, glimepiride 4 mg qam, metformin 1000 mg bid, atenolol, lisinopril, pravachol, asa
81 mg. SMBG FBG 180s, before dinner or HS up to 200s-300s.
c. Decrease precose, add januvia 50 mg qd
Ht: 5’8”, wt 177#. Review of diet indicates patient is not overeating. A1C 11.2, LDL 98, HDL 41, TG 144, TC 177.
Q: Which of the following is the most effective approach to improve JRs glycemic control?
Case Study #3
c. Increase Lantus 1 unit daily until FBG less than
MG42849G TLC MEMBER GUIDE_v2_MG42849G TLC MEMBER GUIDE_v2 6/15REMEMBER TO SHARE THIS GUIDE WITH YOUR DOCTOR. MG42849G TLC MEMBER GUIDE_v2_MG42849G TLC MEMBER GUIDE_v2 6/15 Introduction Welcome to your three-tier outpatient prescription drug plan! Your three-tier drug program gives you access to all medications in coveredclasses within the confines of your plan’s benefit design. This pl
Implementation of Electronic Dividend Payment (“eDividend”) We are pleased to inform you of the provision of eDividend to shareholders, by Jerasia Capital Berhad (“ the Company ”). The eDividend refers to the payment of cash dividends by the Company directly into the shareholders’ bank accounts. One of the main objectives of implementing eDividend is to promote greater effici
 “Making Clinical Sense of Diabetes
“Making Clinical Sense of Diabetes