Copyright c Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Copyright c 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins
Efficacy of Amantadine Treatment onSymptoms and NeurocognitivePerformance Among AdolescentsFollowing Sports-Related Concussion
Cara Camiolo Reddy, MD; Michael Collins, PhD; Mark Lovell, PhD; Anthony P. Kontos, PhDObjective: To evaluate the efficacy of amantadine in the treatment of symptoms and neurocognitive performance in adolescents following sports-related concussion. Participants: A clinical sample of 25 male (n = 11) and female
(n = 14) adolescent subjects with an age-, sex-, and concussion history–matched group of 25 male (n = 11) and
female (n = 14) control subjects. Setting: Outpatient concussion clinic. Intervention: Retrospective, case-control
design. Treatment group consisted of patients treated with 100 mg of amantadine twice daily (200 mg total per day) following a period of rest. Matched controls were evaluated and treated conservatively without medication at the same concussion program prior to the start of the current amantadine protocol. Main Outcome Measures: Immediate Postconcussion Assessment and Cognitive Test computerized neurocognitive test battery and symptom report. Results: Results support significantly greater improvements from pre- to posttest in reported symptoms, verbal memory, and reaction time performance for the amantadine group than the matched controls. There were no significant differences for visual memory or visual motor processing speed. Conclusion: This study provides empirical support for amantadine as an effective pharmacologic treatment of certain concussion-related cognitive deficits and symptoms in athletes with protracted recovery of more than 3 weeks. Key words: amantadine, concussion, postconcussion symptoms
THE pathophysiology of traumatic brain injury lae of TBI. For individuals who have sustained a mild
(TBI) has been postulated to involve complex bio-
TBI, or concussion, these disruptions clinically manifest
chemical cascades leading to dysregulation of ions and
in an array of symptoms including physical, cognitive,
neurotransmitters, as well as increases in inflammatory
emotional, or sleep-related disturbances.2
mediators and free radical production.1 Disruption in
Dopamine, in particular, is known to have strong in-
the release and uptake of neurotransmitters has been
fluences in the frontal lobe and is involved in regulation
considered a likely source of the neurocognitive seque-
of behavior, executive function, judgment, arousal, andmotor control.3 Medications that antagonize dopamin-ergic pathways (eg, haloperidol, risperidone) have re-
Author Affiliations: Departments of Physical Medicine and
sulted in negative consequences for recovery from
Rehabilitation (Dr Camiolo Reddy) and Orthopedic Surgery (Drs Camiolo
TBI.4,5 Conversely, medications that improve dopamin-
Reddy, Collins, Lovell, and Kontos), University of Pittsburgh MedicalCenter, Pittsburgh, Pennsylvania.
ergic transmission (eg, bromocriptine, methylphenidate)have led to improvements in functional outcomes in
The authors thank Rosanna Sabini, DO, and Maria Twichell, MD, Depart-ment of Physical Medicine and Rehabilitation, University of Pittsburgh, for
animal models.6,7 Limited but growing evidence sug-
gests that dopaminergic neurostimulants may facilitate
Drs Camiolo Reddy and Kontos had full access to all of the data in the study
recovery and quality of life for persons with brain injury;
and take responsibility for the integrity of the data and the accuracy of the data
however, no studies to date have addressed the effects
of neurostimulants on athletes following concussion. Michael W. Collins, PhD and Mark R. Lovell, PhD, are stockholders in
Amantadine is a dopaminergic agent that presy-
ImPACT Applications, Inc, the company that develops and sells ImPACT
naptically facilitates the release of dopamine and in-
software. None of the other authors have any financial or other conflicts ofinterests to disclose.
hibits reuptake, thereby increasing the concentrationof dopamine in the synaptic cleft. Amantadine also
Corresponding Author: Cara Camiolo Reddy, MD, Department of Physical Medicine and Rehabilitation, University of Pittsburgh Medical Center, 1400
has a direct postsynaptic effect on dopamine recep-
Locust St D-G103, Pittsburgh, PA 15219
tors that increases density and/or alters their config-
uration. In addition, amantadine is a noncompetitive
Copyright 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Copyright c Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. N-methyl-D-aspartate antagonist that may afford neuro-
treatment group would (1) report a significantly greater
protective effects through inhibition at excitatory gluta-
decrease in symptoms from pre- to posttest and (2) score
significantly better on neurocognitive tests from pre- to
For several decades, amantadine has been used as an
posttest than age-, sex-, and concussion history–matched
antiviral agent and was subsequently found to be effec-
controls. The researchers expected that participants in
tive in the treatment of Parkinson disease.8 Preliminary
the control group would also improve over time, al-
research and anecdotal evidence regarding the use of
though not as much as those in the treatment group.
amantadine for the treatment of neurocognitive deficitsresulting from TBI has been promising, and, as such,
amantadine is often used off label for persons with
mild, moderate, and severe TBI. Recognized as a safeand well-tolerated medication, the potential adverse ef-
The retrospective case-control, pre-/posttest design
fects of amantadine include gastrointestinal upset, in-
used in this study was approved by the institutional
somnia, vivid dreams, anorexia, irritability, agitation,
review board of the University of Pittsburgh.
livedo reticularis, and peripheral edema. These adverseeffects are dose dependent and reversible. Reported ad-
Participants
ministration of amantadine for the treatment of TBI has
A clinical sample of 25 adolescents (11 male, 14 fe-
ranged from 50 to 400 mg daily in divided doses, with
male participants) evaluated and treated at the UPMC
a favorable onset of action of approximately 48 to 72
Sports Medicine Concussion Program constituted the
hours.9 In several case studies and retrospective reviews,
“treatment” participants. They were given 100 mg of
researchers have reported that amantadine improved
amantadine twice daily at breakfast and lunch (200 mg
cognitive function including attention, concentration,
total per day) for an average of 3 to 4 weeks after fail-
processing time, psychomotor speed, sequencing, agita-
ing to recover following a period of rest of approxi-
tion, impulsivity, perseveration, vocalizations, fatigue,
mately 21 days. An age-, sex-, and concussion history–
initiation, participation in therapy, and response to com-
matched group of 25 adolescents evaluated and treated
mands and sensory stimulation.10–17 One small placebo-
conservatively (ie, rest) without medication at the same
controlled double-blind crossover study reported no sta-
clinical concussion program prior to the start of the
tistical effect of amantadine on cognitive function in
current amantadine protocol was selected as controls.
persons with TBI.18 In contrast, another study using
These individuals did not receive any confounding phar-
a similar design and sample reported consistent trends
macologic treatments, and all nonpharmacologic treat-
toward more rapid functional improvement after aman-
ment (ie, education) was consistent between groups.
tadine administration as measured by the Disability Rat-
Inclusion criteria for all were (1) 13 to 19 years of
ing Scale, Glasgow Outcome Scale, and Functional In-
age and (2) a diagnosis of current symptomatic sports-
related concussion. Exclusion criteria were (1) history
To date, there have been no published empirical re-
of migraines, headaches, neurologic disorder, sleep dis-
ports on the use of amantadine in the treatment of
order, or attention-deficit disorder and/or attention-
symptoms and cognitive deficits in athletes following
deficit/hyperactivity disorder; (2) diagnosis of major psy-
concussion. Moreover, in previous literature on the use
chiatric disorder; (3) current, or history of, substance
of amantadine in TBI, most participants were adults,
abuse; (4) contraindications for treatment with amanta-
with varying time periods between injury and therapeu-
dine; or (5) concurrent pharmacologic treatment involv-
tic intervention and heterogeneity in mechanism and
ing medications with known central nervous system or
severity of injury. Therefore, the purpose of the current
symptom-modifying effects. The average age was 15.54
study was to examine changes in symptoms and neu-
(SD = 1.42) years. Demographic and testing informa-
rocognitive performance from pre- to posttreatment in
tion for the treatment and control groups is provided in
a sample of adolescent athletes following concussion.
Table 1. There were no significant group differences on
The treatment group received 100 mg of amantadine
twice daily (200 mg per day) and was compared with agroup of untreated, age-, sex-, and concussion history–
Outcome measures
matched controls. Given the reported neurocognitivebenefits of amantadine for patients with TBI, the re-
All participants completed the Immediate Postcon-
searchers hypothesized that amantadine would be effi-
cussion Assessment and Cognitive Test (ImPACT) com-
cacious in the treatment of postconcussive symptoms
puterized neurocognitive test battery and symptom re-
and cognitive deficits in individuals who have not spon-
port. The ImPACT comprises a series of 6 modules
taneously recovered within 3 weeks from injury. Specifi-
that yield 4 composite scores: verbal memory (% cor-
cally, the researchers hypothesized that the amantadine
rect), visual memory (% correct), visual processing speed
Copyright 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Copyright c Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Amantadine Efficacy in Sports-Related Concussion Among AdolescentsSummary of demographic and test variables for the amantadine (n = 25)treatment and matched control (n = 25) subjects and results of independent sample t testsAmantadine group Control group
(higher number = better performance), and reaction
for medical evaluation and treatment when their symp-
time (in seconds, lower number = better performance).
toms from concussion have not abated within 21 to
The ImPACT also contains a 22-item self-report symp-
30 days postinjury. Pharmacologic treatments are intro-
tom inventory that includes items for problems such as
duced if the athlete has not shown significant signs of
headache, dizziness, memory problems, difficulty con-
recovery within this 3- to 4-week period following in-
centrating, anxiety, depression, and sleep. The concus-
jury, as research from our group indicates that 80% of
sion symptom inventory uses a 7-point Likert-type scale
athletes recover spontaneously within this time.28
in which 0 is a complete absence of symptoms and 6
Those in the treatment group were given 100 mg of
is the most severe.19–21 The ImPACT and symptom re-
amantadine twice daily for 3 to 4 weeks. None discon-
port have been reported to be both valid and reliable in
tinued the medication because of adverse effects. Those
in the control group were not given medication, as theywere admitted to the clinic prior to the implementa-
Procedures
tion of the current medication protocols. Those in bothgroups were tested again using the ImPACT and the
All individuals selected for the study sustained a
symptom report at approximately 40 to 50 days postin-
sports-related concussion and were referred for evalu-
ation to the UPMC Sports Medicine Concussion Pro-gram by an emergency department, high school ath-
Data analysis
letic trainer, or physician. As most were injured whileplaying organized sports, concussions were diagnosed
Repeated-measures analyses of covariance (covaried
initially by certified athletic trainers and/or team physi-
for concussion history) with Bonferroni corrections were
cians present on the sidelines. The basis for diagnosis
used to compare the pre- and posttest ImPACT (ie, ver-
was presentation of 1 or more of the following signs
bal and visual memory, visual processing speed, reaction
or symptoms after a direct or indirect impact to the
time) and symptom scores of the amantadine treatment
head: (1) any noticeable change in mental status; (2) loss
group with the matched controls. All statistical tests were
of consciousness, disorientation, posttraumatic amnesia,
performed using Statistical Package for the Social Sci-
or retrograde amnesia; or (3) any self-reported symp-
ences (SPSS: IBM) version 18. A significance level of P
toms (eg, headache, dizziness, balance dysfunction, vi-
< .05 was used for all statistical tests.
sual blurring, diplopia) that appeared following a direct
or indirect impact to the head. For individuals who werenot injured while playing organized sports, concussions
A series of repeated-measures analyses of covariance
were diagnosed by emergency or family medical person-
(covaried for concussion history at a value of 0.68) sup-
nel and subsequently referred to the clinic for evaluation
ported significant within-subject effects for time across
and treatment. All initial diagnoses were confirmed by
all ImPACT neurocognitive composite scores and re-
clinical personnel (ie, neuropsychologists or physicians)
ported symptoms (Table 2). Specifically, participants in
using the aforementioned description.
both groups reported a decrease in symptoms and an
Following injury, all participants completed a clinical
increase in verbal and visual memory, visual processing
neuropsychological interview that included self-report
speed, and reaction time scores from pre- to posttest.
and information from their parents. At that time, they
There were 3 significant between-group differences at
also completed the pretest ImPACT battery and symp-
the pretest: (1) verbal memory (F1,47 = 7.90, P = .007),
tom report (see Table 1 for average times from injury to
with the amantadine group (M = 72.52, SD = 20.76)
pre- and posttests). It is standard protocol at the UPMC
scoring significantly lower than the controls (M = 84.92,
Sports Medicine Concussion Program to refer patients
SD = 7.57); (2) visual memory (F1,47 = 4.43, P = .04),
Copyright 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Copyright c Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Summary of within-subject effects for time (pre- to posttest) across symptomsand ImPACT composite scores (N = 50)Posttest
with the amantadine group (M = 61.92, SD = 16.37)
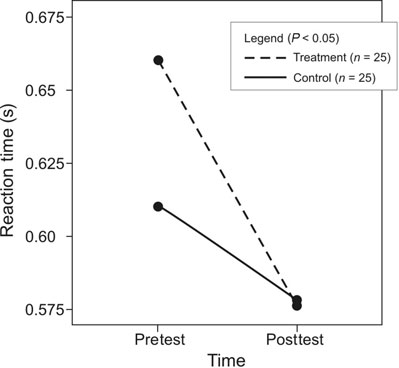
proved (ie, decreased in time [in seconds]) from pre-
scoring significantly lower than the controls (M = 70.08,
to posttest, improvement of the treatment group was
SD = 9.14); and (3) total symptoms (F1, 47 = 6.67,
significantly larger than that of the control group. P = .01), with the amantadine group (M = 37.08,SD = 20.81) scoring significantly higher than the con-
DISCUSSION
trols (M = 23.00, SD = 18.60). There were no significantbetween-group differences at the pretest for processing
Estimates indicate that several million sports- and
speed (P = .18) or reaction time (P = .13). The time
recreation-related concussions occur annually in the
interval between pre- and posttest was 22.8 days (SD =
United States,29 with a majority of patients recovering
26.40) for the amantadine group and 20.2 days (SD =
spontaneously within the first 1 to 3 weeks postin-
30.91) for the control group (t = 0.32, P = 0.75).
jury. Unfortunately, for many individuals, symptoms
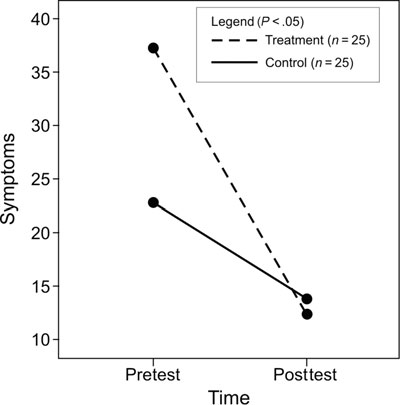
As is evident in Table 3, 3 significant interactions be-
including headaches, dizziness, fogginess, difficulty
tween time (pre- and posttests) and group (treatment and
concentrating, sensitivity to light and noise, irritabil-
controls) were supported for symptoms, verbal mem-
ity, and sleep dysregulation persist beyond the first
ory, and reaction time. The interaction between time
month after injury. These symptoms can be signifi-
and group on symptoms is represented in Figure 1. Al-
cantly disabling, often resulting in an inability to attend
though symptoms of both groups decreased from pre-
school, complete academic work, participate in sporting
to posttest, decrease of the treatment group was larger
and extracurricular activities, and interact socially with
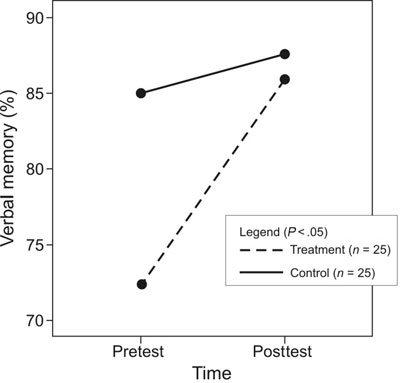
than that of the control group. The interaction between
time and group on verbal memory is represented in
In this study, we retrospectively evaluated a group
Figure 2. Again, although verbal memory performance
of patients treated with amantadine alone and them
of both groups increased from pre- to posttest, increase
compared with an age-, sex-, and concussion history–
of the treatment group was significantly larger than that
matched group of patients who went through the con-
of the control group. The interaction between time and
cussion program prior to the initiation of medication
group on reaction time is represented in Figure 3. Again,
protocols. The control group did not receive any phar-
although reaction time performance of both groups im-
macologic treatment, and neither group received any
Summary of results from the repeated-measures analyses of covariance for theamantadine (n = 25) treatment and matched control (n = 25) subjectsAmantadine group Control group Pre, M (SD) Post, M (SD) Pre, M (SD) Post, M (SD) Wilk λ η2
Copyright 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Copyright c Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Amantadine Efficacy in Sports-Related Concussion Among AdolescentsFigure 3. Reaction time covariate appearing in the model is evaluated at the following value: concussion history = 0.68. Figure 1. Symptom covariate appearing in the model is eval- uated at the following value: concussion history = 0.68.
tive processing and functional improvement when usedin the treatment of TBI. This is the first study to assess
concurrent pharmacologic treatment with known cen-
the use of this medication in the treatment of student
tral nervous system or symptom-modifying effects, in-
athletes following mild TBI or concussion. These re-
cluding medications to treat headaches, sleep, or mood.
sults highlight one possible treatment for the patients
As expected, both groups had significant within-subject
with prolonged recovery from concussion, but the au-
improvements as noted by a decrease in reported symp-
thors recognize and assert that this medication may not
toms and improvements in verbal and visual memory,
be the treatment of choice for all patients with postcon-
visual processing speed, and reaction time from pre- to
cussive symptoms. Individualized concussion treatment
posttest. This indicates natural recovery from concussive
requires in-depth interview to evaluate the symptoms
injury, which is expected to occur over time; however,
and to tailor a management plan based upon each indi-
for those in the amantadine treatment group, the im-
provements in reported symptoms, verbal memory, and
The current study was limited by several factors. Most
reaction time were significantly greater than those found
notably, the sample size was small due to the need to
in their matched controls, suggesting efficacy for aman-
limit the subject pools to patients taking amantadine
tadine in the treatment of these symptoms.
only (treatment group) or no medications at all (matched
These results corroborate prior case reports and anec-
controls); potential participants were excluded from
dotal evidence that amantadine positively affects cogni-
both groups if they had been prescribed any other inter-ventions such as sleep aids, pain relievers, or headachemedications. Nonetheless, the small sample size couldhave resulted in nonrepresentative groups and spuriousfindings. However, the groups were matched on knownfactors that influence concussion outcomes includingage, sex, and concussion history. Although both groupsreceived education as part of our standard managementprotocols, we were unable to control for adherence torest in the amantadine and control groups; however,there is no reason to suggest that either group wouldhave been more or less likely to adhere appropriately. The case-control research design resulted in data thatwere retrospective. Premorbid differences in neurocog-nitive performance and symptoms could have resultedin the within-subject interaction with time reported inthe present study. The nonrandomized design resulted
Figure 2. Verbal memory covariate appearing in the model is
in both participants and clinicians being aware of the
evaluated at the following value: concussion history = 0.68.
use of amantadine. As such, placebo and experimenter
bias (ie, the desire for amantadine efficacy) effects could
Copyright 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Copyright c Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
explain the results of the current study. In summary,
tion time performance in adolescents compared with
the limitations of the current study warrant additional
matched controls. This finding provides tentative sup-
research using a double-blind, randomized control de-
port for the efficacy of amantadine as pharmacologic
sign involving a large sample to substantiate the findings
treatment of patients who fall outside of the normal
recovery trajectory (i.e., >3 weeks) following concus-sion. However, given the small sample size and retro-spective case-control design, the results of this study
CONCLUSION
should be viewed cautiously. The authors advocate for
In the current study, treatment with amantadine re-
double-blind randomized control trials of the efficacy of
sulted in a significant decrease in reported symptoms
amantadine following concussion in a sufficiently large
as well as improvements in verbal memory and reac-
sample to corroborate the findings of this study. REFERENCES
1. Giza CC, Hovda DA. The neurometabolic cascade of concussion.
16. Nickels Schneider WN, Dumbovy ML, Wong TM. Clinical use of
J Athl Train. 2001;36(3):228–235.
amantadine in brain injury rehabilitation. Brain Inj. 1994;8(5):709–
2. Centers for Disease Control and Prevention. What are the signs
17. Meythaler JM, Brunner RC, Johnson A, Novack TA. amantadine
to improve neurorecovery in traumatic brain injury-associated dif-
3. Zafonte RD, Lexell J, Cullen N. Possible applications for dopamin-
fuse axonal injury: a pilot double-blind randomized trial. J Head
ergic agents following traumatic brain injury, part 1. J Head TraumaTrauma Rehabil. 2002;17(4):300–313. Rehabil. 2000;15(5):1179–1182.
18. Schneider WN, Drew-Cates J, Wong TM, Dumbovy ML, et al.
4. Feeney DM, Gonzalez A, Law WA. Amphetamine, haloperidol,
Cognitive and behavioural efficacy of amantadine in acute trau-
and experience interact to affect rate of recovery after motor cortex
matic brain injury: an initial double-blind placebo-controlled
injury. Science. 1982;217(4562):855–857.
study. Brain Inj. 1999;13(11):863–872.
5. Kline AE, Hoffman AN, Cheng JP, Zafonte RD, Massucci JL.
19. Lovell MR, Collins MW, Iverson GL, et al. Recovery from mild
Chronic administration of antipsychotics impede behavioral re-
concussion in high school athletes. J Neurosurg. 2003;98(2):296–
covery after experimental traumatic brain injury. Neurosci Lett.
20. Aubry M, Cantu R, Dvorak J, et al. Summary and agreement
6. Kline AE, Massucci JL, Ma X, Zafonte RD, Dixon CE.
statement of the First International Conference on Concussion in
Bromocriptine reduces lipid peroxidation and enhances spa-
Sport, Vienna 2001. Recommendations for improvement of safety
tial learning and hippocampal neuron survival in a rodent
and health of athletes who may suffer concussive injuries. Br J Sport
model of focal brain trauma. J Neurotrauma. 2004;21(12):1712–
21. Lovell MR, Collins MW. Neuropsychological assessment of the
7. Kline AE, Yan HQ, Bao J, Marion DW, Dixon CE.
college football player. J Head Trauma Rehabil. 1998;13(2):9–26.
Chronic methylphenidate treatment enhance water maze per-
22. Iverson GL, Brooks BL, Lovell MR, Collins MW. Tracking neu-
formance following traumatic brain injury in rats. Neurosci Lett.
ropsychological recovery following concussion in sport. Brain Inj.
8. Chen JJ, Swope DM. Pharmacotherapy for Parkinson’s disease.
23. Iverson GL, Lovell MR, Collins MW. Validity of ImPACT for
Pharmacotherapy. 2007;27(12, pt 2):161S–173S.
measuring processing speed following sports-related concussion. J
9. Zafonte RD, Lexell J, Cullen N. Possible applications for dopamin-
Clin Exp Neuropsychol. 2005;27(6):683–689.
ergic agents following traumatic brain injury: part 2. J Head Trauma
24. Iverson GL, Lovell MR, Collins MW. Interpreting change
Rehabil. 2001;16(1):112–116.
on ImPACT following sport concussion. Clin Neuropsychol.
10. Chandler M, Barnhill J, Gualtieri C. Amantadine for the agitated
head injury patient. Brain Inj. 1998;2(4):309–311.
25. Lau BC, Collins MW, Lovell MR. Sensitivity and specificity of
11. Zafonte R, Watanabe T, Mann N. Amantadine: a potential treat-
subacute computerized neurocognitive testing and symptom eval-
ment for the minimally conscious state. Brain Inj. 1998;12(7):617–
uation in predicting outcomes following sports-related concussion
[published online ahead of print February 7, 2011]. Am J Sports
12. Karli D, Burke DT, Kim HJ, et al. Effects of dopaminer-
gic combination therapy for frontal lobe dysfunction in trau-
26. Lovell MR, Iverson GL, Collins MW, et al. Measurement of
matic brain injury rehabilitation. Brain Inj. 1999;13(1):63–
symptoms following sports-related concussion: reliability and nor-
mative data for the post-concussion scale. Appl Neuropsychol.
13. Beers SR, Skold A, Dixon CE, Adelson PD. Neurobehav-
ioral effects of amantadine after pediatric traumatic brain in-
27. Schatz P, Pardini JE, Lovell MR, Collins MW, Podell K. Sensitiv-
jury: a preliminary report. J Head Trauma Rehabil. 2005;20(5):
ity and specificity of the ImPACT test battery for concussion in
athletes. Arch Clin Neuropsychol. 2006;21(1):91–99.
14. Green LB, Hornyak JE, Hurvitz EA. Amantadine in pediatric
28. Collins MW, Lovell MR, Iverson GL, et al. Cumulative effects of
patients with traumatic brain injury. Am J Phys Med Rehabil.
concussion in high school athletes. Neurosurgery. 2002;51:1175–
15. Kraus MF, Maki P. The combined use of amantadine a l-
29. Langlois JA, Rutland-Brown W, Wald M. The epidemiology and
dopa/carbidopa in the treatment of chronic brain injury. Brain
impact of traumatic brain injury: a brief overview. J Head TraumaRehabil. 2006;21(5):375–378.
Copyright 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
TIA (Transient Ischaemic Attack) Protocol Use only if symptoms < 24 hrs and completely resolved. If brain imaging shows haemorrhage, use Main Stroke Protocol. For supporting information e.g. images & documents, refer to web site at: http://nbsvr73/medicine/StrokeService/StrokeProtocol.html Seek specialist advice for all patients In patients presenting within 1 week of symptom o
Recommended Dog Food Broken Tail Rescue, Inc. believes in the importance of good nutrition for our pets. That’s why we only feed our foster dogs high-quality pet food without by-products, corn and nutrient-lacking fillers. We encourage our adopters to do their own research into different food brands – what you may think is high-quality because of enthusiastic marketing claims may not b
 Copyright c Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Copyright c Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.