Effect of valsartan on left ventricular anatomy and systolic function and aortic elasticity
Available online at www.sciencedirect.com
Metabolism Clinical and Experimental 58 (2009) 682 – 688
Effect of valsartan on left ventricular anatomy and systolic function
Lalita Khaodhiara, Aoife M. Brennanb, Christina Limaa, Jean L. Chanb, Christos S. Mantzorosb,
Warren J. Manningc, Peter G. Daniasd,e, Aristidis Vevesa,⁎
aMicrocirculation Laboratory, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA 02215, USA
bDepartment of Medicine, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA 02215, USA
cDepartment of Radiology, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA 02215, USA
dCardiac MR Center and 2nd Cardiology Clinic, Hygeia Hospital, Maroussi, Athens 15123, Greece
eTufts University School of Medicine, Boston MA 02111, USA
Received 30 July 2008; accepted 21 January 2009
The objective of the study was to examine the effect of a 6-month daily treatment with 160 mg valsartan, an angiotensin II receptor
blocker, on the left ventricular systolic function and aortic elasticity of patients with type 2 diabetes mellitus (T2DM) and healthy subjects. This was a prospective, randomized, double-blind, placebo-controlled crossover study. Thirteen healthy control subjects and 11 patients withT2DM were enrolled in the study. Eight control subjects and 4 T2DM patients completed the study. Cardiovascular magnetic resonance wasused to evaluate the effect of valsartan on the left ventricular function and aortic elasticity. At baseline, T2DM patients had increased leftventricular mass (P = .006) when compared with the healthy controls. In the T2DM patients, treatment with valsartan, in comparison withreceiving placebo, resulted in a reduction of aortic radius (P = .026) and wall thickness (P = .032) of the ascending aorta. In the abdominalaorta, valsartan treatment, when compared with placebo treatment, reduced the arterial compliance (P = .014) in the T2DM patients. Valsartantreatment for 6 months decreased the diameter and wall thickness of the ascending aorta in patients with T2DM, but may decrease AC of theabdominal aorta. 2009 Elsevier Inc. All rights reserved.
be about 5-fold for women This increased risk implies adirect relationship between diabetes and cardiomyopathy
Diabetes is associated with an increased risk for cardiovas-
because it persisted despite controlling for other factors that
cular morbidity and mortality that is considered to be related
could be related to the development of heart failure such as age,
mainly to changes in the lipid profile, accelerated athero-
hypertension, coronary artery disease, lipid abnormalities, and
sclerosis, endothelial dysfunction, increased platelet aggreg-
obesity. The causes of diabetic cardiomyopathy are not clear,
ability, raised fibrogen levels, and increased plasminogen
and there is probably a constellation of pathogenic mechanisms
activator inhibitor–1 activity . Diabetes is also associated
with a distinct cardiomyopathy, the main clinical feature of
Type 2 diabetes mellitus is associated with impaired
which is congestive heart failure in the absence of coronary
vascular elastic properties of the arterial tree, including the
artery, hypertensive, valvular, congenital, or alcoholic heart
large vessels such as the ascending and abdominal aorta
disease Diabetic men participating in the Framingham
Under normal circumstances, the bolus of blood that is
Heart Study had more than twice the risk for development of
propulsed into the arterial system during ventricular ejection
congestive heart failure compared with nondiabetic partici-
creates flow waves that travel distally at a velocity that is
pants. The previously mentioned increased risk was shown to
largely determined by the elastic properties of the arterialwall and the distal conduit resistances, which inducereflectance waves Reduced elasticity is believed to
result in increased systolic pressure and ventricular mass and
Corresponding author. Tel.: +1 617 632 7075; fax: +1 617 632 7090.
0026-0495/$ – see front matter 2009 Elsevier Inc. All rights reserved.
L. Khaodhiar et al. / Metabolism Clinical and Experimental 58 (2009) 682–688
Animal studies indicate that treatment with angiotensin II
receptor blockers (ARB), in combination with angiotensin-converting enzyme inhibitors or alone, has a beneficial effect
This was a prospective, randomized, double-blind,
on cardiac remodeling and ventricular function after
placebo-controlled, crossover study. All participants were
myocardial infarction . These beneficial effects are
evaluated during an initial screening visit and, if suitable,
mediated by nitric oxide in heart failure . There is,
were asked to return and be enrolled in the study. The design
however, little information regarding humans. In addition, no
of the study is depicted in . The randomization process
information is available regarding the effects of angiotensin
occurred within groups; and as a result, it was separated for
II blockade in diabetic patients where ventricular dysfunc-
the 2 groups. The first period lasted 6 months, the washout
period lasted 2 months, and the second period lasted 6
The primary hypothesis of this trial was that indices of left
months. The baseline visit included physical examination,
ventricular (LV) function and aortic elasticity are impaired in
blood tests, and CMR. Participants were randomized at this
diabetes, even in the absence of coronary artery disease, and
visit and were started on treatment with either placebo or 160
that valsartan, an ARB, may improve LV function and aortic
mg valsartan daily. The second visit, at the end of the first 6-
elasticity in the early stages of diabetic cardiomyopathy.
month period, included a physical examination, blood tests,and CMR. The third visit, at the end of the 2-month washoutperiod, included physical examination, blood tests, and
CMR. Each participant was switched to the oppositetreatment of that of the first period. The exit visit included
physical examination, blood tests, and CMR. In all visits,
Twenty healthy nondiabetic subjects and 20 patients with
laboratory tests were performed after an overnight fast.
T2DM, aged 21 to 80 years, were recruited. Healthy
Compliance was evaluated by counting the returned tablets.
nondiabetic subjects underwent an oral glucose tolerance
Plasma glucose, total serum cholesterol, low-density
test to exclude unknown diabetes. Oral fasting glucose of less
lipoprotein cholesterol, high-density lipoprotein cholesterol,
than 100 mg/dL and a 2-hour post–oral glucose tolerance test
triglycerides, liver function tests, electrolytes, blood urea
plasma glucose less than 140 were required Exclusion
nitrogen, and creatinine were measured using the Synchron
criteria included clinical coronary artery disease; arrhythmia;
CX analyzer (Beckman/Coulter, Brea, CA). Hemoglobin A1c
heart failure (New York Heart Association class III and IV);
(HbA1c) (reference range, 4%-6%) was determined in whole
stroke or transient ischemic attack; uncontrolled hyperten-
blood using ion exchange high-performance liquid chroma-
sion; macroalbuminuria; severe dyslipidemia (triglycerides
N600 mg/dL or cholesterol N350 mg/dL); serious chronic
disease that could affect the ability of the subject to participatein the study; treatment with ARBs, glucocorticoids, anti-
Cardiovascular magnetic resonance imaging was per-
neoplastic agents, and bronchodilators; claustrophobia; and
formed on a 1.5-T whole-body scanner (Gyroscan NT/ACS;
subjects unable to have cardiovascular magnetic resonance
Philips Medical Systems, Best, the Netherlands), which is
(CMR) scan (eg, pacemaker, defibrillator).
equipped with the Powertrack 6000 gradient hardware (23
The protocol was approved by the institutional review
mT/m, 219-μs rise time), and advanced cardiac software. A
board at the Beth Israel Deaconess Medical Center. All
5-element phase array coil was used as the radiofrequency
participants gave written informed consent. Participants for
receiver for imaging of the heart and thoracic aorta, and the
the study were recruited through local advertisement.
body coil was used for imaging of the abdominal aorta.
Fig. 1. Scheme of the clinical trial.
L. Khaodhiar et al. / Metabolism Clinical and Experimental 58 (2009) 682–688
After initial localizing “scout” images, cine LV long-axis
P(d)]}, where D(s) and D(d) are the systolic and diastolic
(2-chamber), 4-chamber, and contiguous short-axis images
diameters of the artery and P(s) and P(d) are the systolic
were obtained using a steady-state free processor breath-hold
and diastolic blood pressures, respectively. Arterial
cine sequence. Temporal resolution of the images was 30 to
compliance is measured in square millimeters per kilo-
35 milliseconds, and the duration of the breath-hold was 10 to
12 seconds (depending on the heart rate). Oblique transverse
Stiffness index (SI): defined as the natural logarithm
images were obtained perpendicular to the long axis of the
of the ratio of systolic to diastolic blood pressure
aorta at the sinotubular junction (ascending aorta) and
divided by the circumferential arterial strain (CAS),
immediately proximal (cephalad) to the renal arteries
which is the fractional increase in arterial diameter
(abdominal aorta). Imaging was performed using a retro-
during the cardiac cycle. Thus, SI is a unitless
spective electrocardiographic-gated phase-encoded gradient-
quantity and considered to be relatively independent
echo sequence with the following parameters: field of view,
of blood pressure. SI = ln[P(s)/P(d)]/CAS, where
210 × 300 mm; matrix, 96 × 128; echo time = 6.5
milliseconds; repetition time = 15 milliseconds; flip angle,
Pressure-strain elastic modulus (Ep): defined as the
30°; slice thickness, 6 mm; and velocity encoding, 300 cm/s.
arterial pulse pressure divided by the CAS: Ep = [P(s) −
Finally, to determine aortic wall thickness, a high-resolution
P(d)]/CAS and is measured in kilopascals.
black blood image was obtained at both the ascending
Young elastic modulus (YEM): defined as the ratio of
thoracic and abdominal aorta using a turbo spin-echo (TSE)
stress (force per unit area) to strain and measures arterial
sequence with a dual inversion pulse with the following
stiffness controlling for vessel wall thickness. YEM =
parameters: field of view, 320 × 400 mm; matrix, 336 × 512;
(R/WT){[P(s) − P(d)]/CAS}, where R is the outer
echo time = 20 milliseconds; repetition time equal to the RR
arterial radius and WT is the wall thickness (intima
interval in milliseconds; TSE factor=12; flip angle, 90°; and
plus media). The YEM is measured in kilopascals.
slice thickness, 6 mm. The latter scan was performed during
breath-holding to minimize respiratory artifacts (breath-holdduration of 10-12 seconds). For the phase-encoded images,
The Minitab statistical package (Minitab, State College,
respiratory motion compensation was accomplished by
PA) was used for the statistical analysis. The analysis for the
measuring multiple signal averages (NSA = 4).
effect of valsartan treatment was performed using a parametric
During the examination, blood pressure was noninva-
test (ie, paired t test) for normally distributed data and a
sively measured using an automated sphygmomanometer
nonparametric test (ie, Wilcoxon matched-pair signed rank
(Dinamap; GE Medical Systems, Madison, WI), with the
test) for data that are not distributed normally to compare the
cuff placed at the calf. The mean of 3 values was used for
changes during the placebo and active period treatments in
calculations of vascular elasticity.
each group. The t test was used to compare the baseline
Image data were transferred off-line to a ViewForum
characteristics between the healthy nondiabetic subjects and
workstation (Philips Medical Systems) for further analysis.
the T2DM patients for normally distributed data and the
Left and right ventricular endocardial and epicardial
Mann-Whitney for nonparametric data. The results are
contours for all short-axis end-diastolic and end-systolic
presented as mean ± SD for normally distributed data and
images were manually traced. Using the commercially
median (25-75 percentile) for data that are not distributed
available analysis package, volumetric assessment of mass,
normally. Single and multiple regression analysis was also
end-diastolic and end-systolic volumes, ejection fraction
performed. Statistical significance was accepted at the 95%
(EF), stroke volume, and cardiac output were derived for the
Aortic maximal and minimal cross-sectional areas were
determined from the phase-encoded flow scans using
semiautomated ViewForum software. Thus, the phases
3.1. Comparisons in CMR measurements between healthy
with the maximal and minimal aortic diameter/area were
determined and used in the calculations for aortic elasticity. For assessment of the aortic wall thickness, 2 measurements
Thirteen healthy control subjects and 11 patients with
were obtained in areas free of artifact; and the mean of the 2
T2DM were enrolled. The baseline demographics of those
who completed the study in each group are shown in
Vascular elasticity was described with the follow-
Type 2 diabetes mellitus patients had higher body mass index
(BMI) (P = .002), systolic blood pressure (P = .03), fastingblood glucose (P = .0001), and HbA1c (P = .0001). Baseline
Arterial compliance (AC): defined as the absolute volume
CMR data are shown in The T2DM patients had
increase within an arterial segment during the cardiac
higher LV mass (P = .006). When all subjects were
cycle divided by the arterial pulse pressure. The AC per
considered as 1 group, significant correlations were found
unit length (1 mm) is AC = π[D(s)2 − D(d)2]/{4[P(s) −
between LV mass and HbA1c (r = 0.58, P = .005), fasting
L. Khaodhiar et al. / Metabolism Clinical and Experimental 58 (2009) 682–688
between changes observed during the valsartan and placebo
treatment periods in both the healthy control subjects and the
T2DM patients. In the ascending aorta measurements of
T2DM patients who completed the study, treatment with
valsartan, in comparison with receiving placebo, resulted in a
reduction of aortic radius (P = .026) and wall thickness (P =
.032). In the abdominal aorta, valsartan treatment, when
compared with placebo treatment, reduced the AC (P = .014)
The main finding of this study is that administration of 160
mg of valsartan, an ARB, for 6 months decreased the radius
and wall thickness of the ascending aorta in T2DM patients,
whereas it had no measurable effects in healthy control
subjects. In the abdominal aorta, valsartan decreased the AC
in the T2DM patients, but had no effect in the controls.
Previous studies have suggested that the development of
cardiomyopathy starts early in the course of diabetes and that
diabetic patients without any clinical findings suggestive of
heart failure may have significant abnormalities of both
systolic and diastolic function In the present study,
we included T2DM patients with no clinical cardiovascular
Mean ± SD or median (25:75 percentile). BP indicates blood pressure; LDL,
low-density lipoprotein; HDL, high-density lipoprotein; BUN, blood urea
nitrogen; ACE, angiotensin-converting enzyme; NS, not significant.
blood glucose (r = 0.53, P = .008), and BMI (r = 0.64, P =
.001); but in multiple regression analysis, only BMI retained
statistical significance. There were no differences in any of
3.2. Effects of valsartan treatment on CMR measurements in
T2DM patients and the healthy control subjects
Eight control subjects and 4 T2DM patients completed
the study. Five subjects were lost to follow-up, 6 subjects
withdrew consent because they were unable to comply with
the study protocol, and 1 subject withdrew because of mild
dizziness that resolved after stopping the study medication. There were no differences between those who completed the
study and those who failed to complete the study in any of
the clinical characteristics that are listed in .
Treatment with valsartan did not have any effect on
systolic and diastolic blood pressure, fasting blood glucose
levels, and HbA1c in both groups. The comparison between
difference in the CMR measurements during the valsartan
and placebo period treatment is shown in There
Data are presented as mean ± SD or median (25:75 percentiles). EDV indicates
were no differences in all performed cardiac measurements
end-diastolic volume; ESV, end-systolic volume; MR, mitral regurgitant.
L. Khaodhiar et al. / Metabolism Clinical and Experimental 58 (2009) 682–688
Table 3Changes with the valsartan treatment when compared with changes during placebo treatment period in the healthy controls and the T2DM patients
Data are presented as mean and 95% confidence intervals.
disease and a relatively short duration of diabetes (mean, 5 ±
sclerosis, this finding, if confirmed at a larger cohort, may
3 years); but our results are in agreement with the previous
be very important because it indicates a possible beneficial
studies because we found that the diabetic patients had
pleiotropic effect of valsartan on atherosclerosis, poten-
increased wall thickness and LV mass when compared with
tially independent of reduction of the peripheral blood
There are very limited data regarding the effect of ARBs
An unexpected finding was the decrease of AC, which is
on cardiac function in diabetes. A recent study that
defined as the absolute volume increase within an arterial
included diabetic patients without hypertension or heart
segment during the cardiac cycle divided by the arterial
disease who were treated for 6 months with candesartan,
pulse pressure, in the abdominal aorta of the valsartan-
another ARB, showed an improvement in diastolic
treated T2DM patients. The calculation of compliance is
dysfunction and attenuation of myocardial fibrosis, sug-
based on the measurement of both the systolic and diastolic
gesting that ARBs may regulate collagen turnover by
aortic diameter and blood pressure. Although CMR can
facilitating collagen degradation Previous studies in
accurately measure changes in the aortic diameter during
our unit have shown that valsartan treatment for 3 months,
valsartan treatment, previous studies have indicated that
at the same dose as in the present study, results in
changes in the central blood pressure are not reflected by
considerable improvement of blood flow in the skin
changes in the peripheral blood pressure measurements;
microcirculation of diabetic patients but had no effect in
and this may be the main reason for the obtained results
the skin microcirculation of healthy control subjects .
. Furthermore, all other indices of vascular elasticity
Furthermore, the same studies indicated that valsartan
were not affected; and there are no pathophysiologic
exerts its beneficial effects by reducing the activity of poly
mechanisms that would explain such deterioration in
(adenosine diphosphate-ribose) polymerase, which is
vascular compliance. As a result, we believe that the
increased in diabetes and is associated with endothelial
physiologic significance of this finding is doubtful. Never-
theless, this finding deserves further investigation in a
The most interesting finding of the present study was
larger sample of patients and possibly during longer periods
the effect of valsartan on the elasticity of the ascending
aorta. In the T2DM patients, valsartan reduced the vessel
In the present study, we have used CMR for evaluating
radius and wall thickness of the ascending aorta. As the
the effect of valsartan on LV function and aortic elasticity.
above measurements are correlates of subclinical athero-
The main reason for this is that this technique is currently
L. Khaodhiar et al. / Metabolism Clinical and Experimental 58 (2009) 682–688
considered as the “criterion standard” for measurement of LV
[5] Kannel WB, Hjortland M, Castelli WP. Role of diabetes in
mass and volumes [Because of extremely high
congestive heart failure: the Framingham Study. Am J Cardiol1974;34:29-34.
accuracy and reproducibility, CMR allows for high statistical
[6] Zarich SW, Nesto RW. Diabetic cardiomyopathy. Am Heart J 1989;
power to detect small differences in cardiac structure and
function between study groups, with even a small sample
[7] Henry RM, Kostense PJ, Spijkerman AM, Dekker JM, Nijpels G,
size. Accordingly, for clinical trials, CMR compares
Heine RJ, et al. Hoorn Study. Arterial stiffness increases with
favorably to echocardiography and is becoming the
deteriorating glucose tolerance status: the Hoorn Study. Circulation2003;107:2089-95.
dominant imaging modality in cardiovascular clinical
[8] Lehmann ED, Watts GF, Fatemi-Langroudi B, Gosling RG. Aortic
research Cardiovascular magnetic resonance can
compliance in young patients with heterozygous familial hypercho-
also most accurately measure small changes in the aortic
lesterolaemia. Clin Sci (Lond) 1992;83:717-21.
lumen cross-sectional area with very high temporal resolu-
[9] O'Rourke MF, Staessen JA, Vlachopoulos C, Duprez D, Plante GE.
tion and can quantify blood flow through large vessels.
Clinical applications of arterial stiffness; definitions and referencevalues. Am J Hypertens 2002;15:426-44.
Therefore, CMR is uniquely suited for the evaluation of the
[10] Groenink M, de Roos A, Mulder BJ, Spaan JA, van der Wall EE.
Changes in aortic distensibility and pulse wave velocity assessed with
The current study has its limitations, of which the most
magnetic resonance imaging following beta-blocker therapy in the
prominent is the considerable number of subjects who did
Marfan syndrome. Am J Cardiol 1998;82:203-8.
not complete the study (9; 37% of the participants). We
[11] Westerhof N, O'Rourke MF. Haemodynamic basis for the development
of left ventricular failure in systolic hypertension and for its logical
believe that the main reason for this was the long duration
therapy. J Hypertens 1995;13:943-52.
of the study and the crossover design. This, combined with
[12] Mankad S, d'Amato TA, Reichek N, McGregor WE, Lin J, Singh D,
the small number of subjects that were recruited, resulted in
et al. Combined angiotensin II receptor antagonism and angiotensin-
a rather small study cohort. However, the fact that valsartan
converting enzyme inhibition further attenuates postinfarction left
was found to improve certain indexes of ascending aortic
ventricular remodeling. Circulation 2001;103:2845-50.
[13] Kim S, Yoshiyama M, Izumi Y, Kawano H, Kimoto M, Zhan Y, et al.
function in T2DM patients but not in controls indicates that,
Effects of combination of ACE inhibitor and angiotensin receptor
despite these limitations, the study has accomplished its
blocker on cardiac remodeling, cardiac function, and survival in rat
primary scope, which was to provide proof of concept and
heart failure. Circulation 2001;103:148-54.
justify the conduction of additional studies in the future. As
[14] Liu YH, Xu J, Yang XP, Yang F, Shesely E, Carretero OA. Effect of
the conduction of such studies is cumbersome and carries a
ACE inhibitors and angiotensin II type 1 receptor antagonists onendothelial NO synthase knockout mice with heart failure. Hyperten-
heavy cost, we believe that the initial conduction of a small
study that aims primarily to provide proof of concept is
[15] American Diabetes Association. Report of the Expert Committee on
fully justified and that the current study has achieved its
the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care
In summary, our results indicate that valsartan treatment
[16] Kahn JK, Zola B, Juni JE, Vini AI. Radionuclide assessment of left
ventricular diastolic filling in diabetes mellitus with and without
for 6 months decreased the diameter and wall thickness of
cardiac autonomic neuropathy. J Am Coll Cardiol 1986;7:1303-9.
the ascending aorta in T2DM patients but may decrease AC
[17] Airaksinen KEJ, Koistinen MJ, Ikaheimo MJ, et al. Augmentation of
atrial contribution to left ventricular filling in IDDM subjects asassessed by Doppler echocardiography. Diabetes Care 1989;12:
[18] Danias PG, Tritos NA, Stuber M, Kissinger KV, Salton CJ, Manning
WJ. Cardiac structure and function in the obese: a cardiovascular
The present study was an investigator-initiated research
magnetic resonance imaging study. J Cardiovasc Magn Reson 2003;5:
protocol and was supported by a clinical research grant to
Aristidis Veves, MD, from Novartis. This research was also
[19] Friberg P, Allansdotter-Johnsson A, Ambring A, Ahl R, Arheden H,
supported in part by grant RR 01032 to the Beth Israel
Framme J, et al. Increased left ventricular mass in obese adolescents.
Deaconess Medical Center General Clinical Research Center
[20] Kawasaki D, Kosugi K, Waki H, Yamamoto K, Tsujino T, Masuyama
from the National Institutes of Health.
T. Role of activated renin-angiotensin system in myocardial fibrosisand left ventricular diastolic dysfunction in diabetic patients—reversal
by chronic angiotensin II type 1A receptor blockade. Circ J 2007;71:524-9.
[1] Deliargyris EN, Nesto RW. Autonomic neuropathy and heart disease.
[21] Shrikhande G, Khaodhiar L, Scali S, Lima C, Hubbard M, Dudley K,
In: Veves A, editor. The clinical management of diabetic neuropathy.
et al. Valsartan improves resting skin blood flow in type 2 diabetic
Totowa (NJ): Humana Press; 1998. p. 209-26.
patients and reduces poly(adenosine diphosphate-ribose) polymerase
[2] Stamler J, Vaccaro O, Neaton J, Wentworth D. Diabetes, other risk
activation. J Vasc Surg 2006;43:760-70.
factors, and 12-yr cardiovascular mortality for men screened in the
[22] Szabó C, Zanchi A, Komjáti K, Pacher P, Krolewski AS, Quist WC,
Multiple Risk Factor Intervention Trial. Diabetes Care 1993;16:434-44.
et al. Poly(ADP-Ribose) polymerase is activated in subjects at risk of
[3] Rubler S, Dlugash J, Yuceoglu YZ, Kumral T, Branwood AW,
developing type 2 diabetes and is associated with impaired vascular
Grishman A. New type of cardiomyopathy associated with diabetic
reactivity. Circulation 2002;106:2680-6.
glomerulosclerosis. Am J Cardiol 1972;30:595-602.
[23] Garcia Soriano F, Virag L, Jagtap P, Szabo E, Mabley JG, Liaudet L,
[4] Raman M, Nesto RW. Heart disease in diabetes mellitus. Endocrinol
et al. Diabetic endothelial dysfunction: the role of poly (ADP-ribose)
polymerase activation. Nat Med 2001;7:108-13.
L. Khaodhiar et al. / Metabolism Clinical and Experimental 58 (2009) 682–688
[24] Danias PG, Tritos NA, Stuber M, Botnar RM, Kissinger KV, Manning
by the use of cardiovascular magnetic resonance. J Cardiovasc Magn
WJ. Comparison of aortic elasticity determined by cardiovascular
magnetic resonance imaging in obese versus lean adults. Am J Cardiol
[29] Stuber M, Nagel E, Fischer SE, et al. Quantification of the local heart
wall motion by magnetic resonance myocardial tagging. Comput Med
[25] Williams B, Lacy PS, Thom SM, Cruickshank K, Stanton A, Collier D,
et al. Differential impact of blood pressure–lowering drugs on central
[30] Fischer SE, McKinnon GC, Scheidegger MB, et al. True myocardial
aortic pressure and clinical outcomes: principal results of the Conduit
motion tracking. Magn Reson Med 1994;31:401-13.
Artery Function Evaluation (CAFE) Study. Circulation 2006;113:
[31] Stuber M, Manning WJ. CSPAMM assessment of left ventricular
diastolic function. In: Manning WJ, Pennell DJ, editors. Clinical
[26] Cranney GB, Lotan CS, Dean L, Baxley W, Bouchard A, Pohost GM.
cardiac magnetic resonance imaging. Churchill Livingstone; 2002.
Left ventricular volume measurement using cardiac axis nuclear
magnetic resonance imaging. Validation by calibrated ventricular
[32] Resnick LM, Militianu D, Cunnings AJ, Pipe JG, Evelhoch JL, Soulen
angiography. Circulation 1990;82:154-63.
RL. Direct magnetic resonance determination of aortic distensibility in
[27] Sakuma H, Fujita N, Foo TK, et al. Evaluation of left ventricular
essential hypertension: relation to age, abdominal visceral fat, and in
volume and mass with breath-hold cine MR imaging. Radiology 1993;
situ intracellular free magnesium. Hypertension 1997;30:654-9.
[33] Rogers WJ, Hu YL, Coast D, Vido DA, Kramer CM, Pyeritz RE, et al.
[28] Bellenger NG, Davies LC, Francis JM, Coats AJ, Pennell DJ.
Age-associated changes in regional aortic pulse wave velocity. J Am
Reduction in sample size for studies of remodeling in heart failure
Parasite Resistance in US Cattle Donald H. Bliss1, PhD; Robert D. Moore2, MS; William G. Kvasnicka3, DVM 1Veterinary Parasitologist, MidAmerica Ag Research, 3705 Sequoia Trail, Verona, WI 53593 2College of Agriculture, Biotechnology & Natural Resources, University of Nevada, Reno, NV 89557 37131 Meadow View, Shawnee, KS 66227 Abstract s’ensuivre à l’insu des producteurs sa
Contact: Pauline O’Keeffe The Schawbel Corporation 781-541-6900 pauline@thermacell.net WHEN IT COMES TO MOSQUITOES, WHICH REPELLENT WORKS BEST? Consumers Learn Repellent Lingo as Mosquito-Borne Illnesses Flourish With West Nile Virus and Eastern Equine Encephalitis (Triple E) continuing to be prevalent in the United States, consumers want and need to become more familia
 Available online at www.sciencedirect.com
Metabolism Clinical and Experimental 58 (2009) 682 – 688
Effect of valsartan on left ventricular anatomy and systolic function
Lalita Khaodhiara, Aoife M. Brennanb, Christina Limaa, Jean L. Chanb, Christos S. Mantzorosb,
Warren J. Manningc, Peter G. Daniasd,e, Aristidis Vevesa,⁎
aMicrocirculation Laboratory, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA 02215, USA
bDepartment of Medicine, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA 02215, USA
cDepartment of Radiology, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA 02215, USA
dCardiac MR Center and 2nd Cardiology Clinic, Hygeia Hospital, Maroussi, Athens 15123, Greece
eTufts University School of Medicine, Boston MA 02111, USA
Received 30 July 2008; accepted 21 January 2009
The objective of the study was to examine the effect of a 6-month daily treatment with 160 mg valsartan, an angiotensin II receptor
blocker, on the left ventricular systolic function and aortic elasticity of patients with type 2 diabetes mellitus (T2DM) and healthy subjects.
Available online at www.sciencedirect.com
Metabolism Clinical and Experimental 58 (2009) 682 – 688
Effect of valsartan on left ventricular anatomy and systolic function
Lalita Khaodhiara, Aoife M. Brennanb, Christina Limaa, Jean L. Chanb, Christos S. Mantzorosb,
Warren J. Manningc, Peter G. Daniasd,e, Aristidis Vevesa,⁎
aMicrocirculation Laboratory, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA 02215, USA
bDepartment of Medicine, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA 02215, USA
cDepartment of Radiology, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA 02215, USA
dCardiac MR Center and 2nd Cardiology Clinic, Hygeia Hospital, Maroussi, Athens 15123, Greece
eTufts University School of Medicine, Boston MA 02111, USA
Received 30 July 2008; accepted 21 January 2009
The objective of the study was to examine the effect of a 6-month daily treatment with 160 mg valsartan, an angiotensin II receptor
blocker, on the left ventricular systolic function and aortic elasticity of patients with type 2 diabetes mellitus (T2DM) and healthy subjects.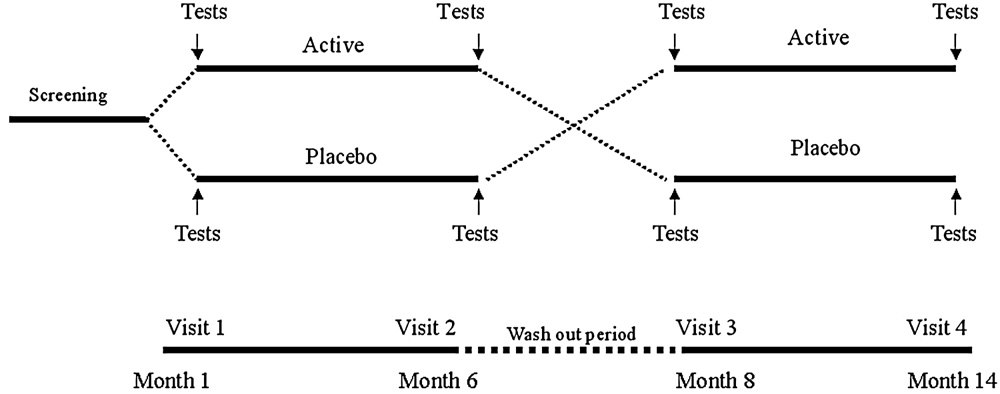 L. Khaodhiar et al. / Metabolism Clinical and Experimental 58 (2009) 682–688
Animal studies indicate that treatment with angiotensin II
receptor blockers (ARB), in combination with angiotensin-converting enzyme inhibitors or alone, has a beneficial effect
This was a prospective, randomized, double-blind,
on cardiac remodeling and ventricular function after
placebo-controlled, crossover study. All participants were
myocardial infarction . These beneficial effects are
evaluated during an initial screening visit and, if suitable,
mediated by nitric oxide in heart failure . There is,
were asked to return and be enrolled in the study. The design
however, little information regarding humans. In addition, no
of the study is depicted in . The randomization process
information is available regarding the effects of angiotensin
occurred within groups; and as a result, it was separated for
II blockade in diabetic patients where ventricular dysfunc-
the 2 groups. The first period lasted 6 months, the washout
period lasted 2 months, and the second period lasted 6
The primary hypothesis of this trial was that indices of left
months. The baseline visit included physical examination,
ventricular (LV) function and aortic elasticity are impaired in
blood tests, and CMR. Participants were randomized at this
diabetes, even in the absence of coronary artery disease, and
visit and were started on treatment with either placebo or 160
that valsartan, an ARB, may improve LV function and aortic
mg valsartan daily. The second visit, at the end of the first 6-
elasticity in the early stages of diabetic cardiomyopathy.
L. Khaodhiar et al. / Metabolism Clinical and Experimental 58 (2009) 682–688
Animal studies indicate that treatment with angiotensin II
receptor blockers (ARB), in combination with angiotensin-converting enzyme inhibitors or alone, has a beneficial effect
This was a prospective, randomized, double-blind,
on cardiac remodeling and ventricular function after
placebo-controlled, crossover study. All participants were
myocardial infarction . These beneficial effects are
evaluated during an initial screening visit and, if suitable,
mediated by nitric oxide in heart failure . There is,
were asked to return and be enrolled in the study. The design
however, little information regarding humans. In addition, no
of the study is depicted in . The randomization process
information is available regarding the effects of angiotensin
occurred within groups; and as a result, it was separated for
II blockade in diabetic patients where ventricular dysfunc-
the 2 groups. The first period lasted 6 months, the washout
period lasted 2 months, and the second period lasted 6
The primary hypothesis of this trial was that indices of left
months. The baseline visit included physical examination,
ventricular (LV) function and aortic elasticity are impaired in
blood tests, and CMR. Participants were randomized at this
diabetes, even in the absence of coronary artery disease, and
visit and were started on treatment with either placebo or 160
that valsartan, an ARB, may improve LV function and aortic
mg valsartan daily. The second visit, at the end of the first 6-
elasticity in the early stages of diabetic cardiomyopathy.