Int. J. Radiation Oncology Biol. Phys., Vol. 46, No. 1, pp. 221–230, 2000
Copyright 2000 Elsevier Science Inc. PII S0360-3016(99)00351-X THE AMERICAN BRACHYTHERAPY SOCIETY RECOMMENDATIONS FOR PERMANENT PROSTATE BRACHYTHERAPY POSTIMPLANT DOSIMETRIC ANALYSIS
SUBIR NAG, M.D.,*† WILLIAM BICE, PH.D.,*‡ KEITH DEWYNGAERT, PH.D.,*§
BRADLEY PRESTIDGE, M.D.,* RICHARD STOCK, M.D.,*¶ AND YAN YU, PH.D.*#
*Clinical Research Committee, The American Brachytherapy Society, Oak Brook, IL; †Ohio State University, Columbus, OH;
‡University of Texas Health Science Center,San Antonio, TX; §New York University, New York, NY; Cancer Therapy and Research
Center, San Antonio, TX; ¶Mt. Sinai Hospital, New York, NY; and #University of Rochester, Rochester, NY
Purpose: The purpose of this report is to establish guidelines for postimplant dosimetric analysis of permanent prostate brachytherapy. Methods: Members of the American Brachytherapy Society (ABS) with expertise in prostate dosimetry evalu- ation performed a literature review and supplemented with their clinical experience formulated guidelines for performing and analyzing postimplant dosimetry of permanent prostate brachytherapy. Results: The ABS recommends that postimplant dosimetry should be performed on all patients undergoing permanent prostate brachytherapy for optimal patient care. At present, computed tomography (CT)-based dosimetry is recommended, based on availability cost and the ability to image the prostate as well as the seeds. Additional plane radiographs should be obtained to verify the seed count. Until the ideal postoperative interval for CT scanning has been determined, each center should perform dosimetric evaluation of prostate implants at a consistent postoperative interval. This interval should be reported. Isodose displays should be obtained at 50%, 80%, 90%, 100%, 150%, and 200% of the prescription dose and displayed on multiple cross-sectional images of the prostate. A dose-volume histogram (DVH) of the prostate should be performed and the D (dose to 90% of the prostate gland) reported by all centers. Additionally, the D the fractional V (i.e., the percentage of prostate volume receiving 80%, 90%, 100%, 150%, and 200% of the prescribed dose, respectively), the rectal, and urethral doses should be reported and ultimately correlated with clinical outcome in the research environment. On-line real-time dosimetry, the effects of dose heterogeneity, and the effects of tissue heterogeneity need further investigation. Conclusion: It is essential that postimplant dosimetry should be performed on all patients undergoing permanent prostate brachytherapy. Guidelines were established for the performance and analysis of such dosimetry. 2000 Elsevier Science Inc. Prostate neoplasm, Brachytherapy, Dosimetry, Guidelines, 125Iodine, 103Palladium. INTRODUCTION
for, and role of postimplant dosimetry following permanentradioactive seed implantation is occasionally questioned.
Postimplant dosimetric analysis is standard practice follow-
This prompted the ABS to organize a panel with expertise in
ing temporary brachytherapy procedures. Its role following
the field of implant evaluation to perform a literature review
permanent implants is less well established. Previous sur-
and to share their experience and knowledge to develop
veys have shown wide variation in dosimetric methods (1,
guidelines for the performance and analysis of postimplant
2); however, there are no established clinical standards or
guidelines for performing prostate dosimetry. The recently
Because the treatment plan and the actual implant have
issued American Brachytherapy Society (ABS) guidelines
already been completed at the time of postimplant analysis,
for prostate brachytherapy recognized the need for such
the rationale for its use needs elucidation. The first issue
guidelines (3). Although an increasing number of prostate
arises from the fact that brachytherapy is an imperfect
brachytherapy procedures are performed annually, the need
modality, and certainly, the permanent ultrasound-guided
Reprint requests to: Subir Nag, M.D., Chief of Brachytherapy,
Brachytherapy Society, and thank Drs. Patrick Swift, Mack Roach,
The Ohio State University, 300 West 10th Avenue, Columbus, OH
Frank Waterman, David Beyer, and Michael Zelefsky for their
43210. Tel: (614) 293-8415; Fax: (614) 293-4044; E-mail:
Presented at the annual meeting of the American Society for
Acknowledgments—The authors wish to express their gratitude to
Therapeutic Radiology and Oncology, San Antonio, TX, Novem-
Mr. David Carpenter for editorial assistance. The authors acknowl-
edge the support of the Board of Directors of the American
Accepted for publication 6 August 1999.
I. J. Radiation Oncology ● Biology ● Physics
prostate implant technique is no exception. The dose distri-
Table 1. Relative advantages and disadvantages of each imaging
butions following implantation are not the same as those
modality for performing post implant dosimetric analysis*
planned prior to the implant (4–10). Because the dose dis-
tributions differ, it is important to document the actual dosethat the prostate and normal adjacent tissues will receive
over the life of the implant. This can only be determined if
a postimplant dosimetric assessment is performed.
The information obtained is essential for optimal patient
care. Significant underdosing of the prostate, which can lead
to treatment failure, can be potentially rectified using sup-
plemental external beam irradiation or additional seed im-
* Grading scale: ϩϩ, ϩ, 0, Ϫ and ϪϪ, where ϩϩ is the
plantation (11). In patients who experience a biopsy-proven
highest ranking and ϪϪ is the lowest.
local failure, the knowledge of the original dose distribution
† MRI (magnetic resonance imaging) performed with a body
may prove useful when considering salvage therapy,
whether in the form of external beam irradiation reimplan-
CT ϭ computed tomography; TRUS ϭ transrectal ultrasound.
tation or radical prostatectomy (12–14). This information isalso important in determining the cause of potential com-
as their spatial relationship from the cross-sectional images.
plications and appropriate patient management
While the advantages of this type of dosimetry over plane
Postimplant dosimetry is invaluable for those physicians
film are overwhelming, each of the above imaging modal-
who are just starting to perform permanent seed implants.
ities has limitations. Table 1 summarizes their relative ad-
Dosimetry results can help physicians assess and modify
vantages and disadvantages. This has prompted efforts to
their implant technique. This is essential because there is a
combine imaging methods by spatially coregistering (i.e.,
learning curve involved in performing prostate brachyther-
fusing) the information from two or more imaging modal-
apy (15, 16). In addition, experienced physicians can use
dosimetry to further refine and perfect the procedure (17).
Historically, the earliest method was plain film dosime-
Finally, the data that is provided by postimplant dosim-
try. The geometric reconstruction of source locations from
etry could be used in future outcome analysis. It would
two projection radiographs has been used for many years to
allow comparison of treatment results from various institu-
perform pre- and postimplant dosimetry. Techniques are
tions and could be used as a quality assurance tool in
available for using films with a common axis and for those
prospective multi-institutional clinical trials.
taken with a stereo shift (19, 20). Methods of correcting forfilm skew—films not perpendicular to the axis of the x-raysource—have been developed (21). The errors inherent in
these methods have been studied (22–24). Unfortunately,
Members of the ABS with expertise in prostate dosimetry
two-film techniques may be used reliably only when the
evaluation performed a literature review, and supplemented
operator is able to match each individual source from one
with their clinical experience, formulated guidelines for
film with its corresponding image on the other film. Because
performing and analyzing postimplant dosimetry for perma-
of the number seeds and their irregular spacing, this is
nent prostate brachytherapy. The areas of consensus and
extraordinarily difficult in permanent prostate brachyther-
controversy were noted. Specific dosimetric recommenda-
tions (for use in a community setting as well as in the
To address this problem, three film techniques have been
research environment) and directions for future investiga-
developed (25–27). These methods dramatically improve
tions were made. This report was reviewed and approved by
the accuracy of seed localization in permanent prostate
implants, achieving true localization rates on the order of90% (28). Radiographs or fluoroscopy can be performed inthe operating room during or immediately after the implant
with equipment that is readily available. Available modalities for obtaining postimplant dosimetry
The principal disadvantage of plane film techniques is
Methods of performing postimplant evaluation of pros-
that they cannot be used to visualize the target (prostate
tate implants can be best categorized by the modality used
gland) and critical structures (rectum, urethra, bladder).
to generate the images. The brachytherapist is no longer
While the dose distribution may be computed and displayed
limited to using plane films. Initially developed for com-
in axial planes, or even viewed as a three-dimensional (3D)
puted tomography (CT) (18), prostate brachytherapy dosim-
object, there is no information about the spatial relationship
etry based upon axial images has been applied to magnetic
of this distribution to the prostate or adjacent structures.
resonance imaging (MRI), and transrectal ultrasound
While other deficiencies exist with this method (organ mo-
(TRUS). The term cross-sectional image set will be used to
tion between films, for instance), it is this shortcoming that
refer generically to all three. Each modality allows, at least
led to the development of cross-sectional image set dosim-
to some degree, localization of structures and seeds, as well
etry such as CT-based dosimetry.
Prostate postimplant dosimetry ● S. NAG et al.
CT-based dosimetry was first applied to prostate implants
implantation of the gland (14). The seed locations are very
by Roy et al. at Memorial Sloan-Kettering Cancer Center in
difficult to discern, and their disruption of the ultrasound
New York (18). The advantage of being able to visualize
signal makes delineation of the prostatic borders more dif-
sources in relation to the target became immediately appar-
ficult than with the preimplant ultrasound. Because of this,
ent, particularly with regard to low energy isotopes such as
it seems unlikely that ultrasound can be used as a single
125I and 103Pd, for which the dose distribution is highly
modality for postimplant dosimetric analysis, unless ultra-
dependent on precisely locating the seed positions. In this
sound technology is improved. The patient discomfort as-
technique, abutting slices taken through the gland were
sociated with this examination particularly after surgery
displayed and digitized into the treatment planning system.
adds to the disadvantages of this option unless the dosimetry
Because the sources often appeared on more than one slice,
is performed on-line, during surgery.
a seed location reduction method (seed sorting) based upon
Nevertheless, there are some features of TRUS that make
it appealing. Ultrasound examination is relative easy and
The basic methods of CT-based implant dosimetry have
inexpensive. The possibility of using the same imaging
changed little. Various authors have published techniques
modality that was used to perform the preplan and the
that adjust the slice spacing or the distance between slices,
implant procedure to generate the post plan is enticing.
and the task of seed sorting has been automated (28).
TRUS potentially offers the only practical option for per-
Properly performed, the accuracy of seed location is on par
forming on-line dosimetric analysis during the procedure,
with, if not superior to, three-film techniques (28, 29).
allowing the brachytherapist to adjust the dose distribution
Limitations of this technique include the required a priori
by adding seeds in regions where the dose is inadequate.
knowledge of the number of seeds in the image set at the
Like MRI, longitudinal imaging is also possible.
beginning of the sorting process. This information can be
Because each imaging modality offers it own advantages,
garnered from a single plane film, usually taken in the
some authors have combined imaging techniques to opti-
anterior-posterior direction, or less reliably, from documen-
mize the information available for the postimplant analysis
tation detailing the number of sources implanted within the
(31, 33, 34). Combining two or more modalities usually
patient. Additionally, some inherent uncertainty is intro-
involves using a modality that optimizes source localization
duced when the location of the seeds in the axial (i.e.,
and another that best delineates the prostatic and critical
cranio-caudal) direction is determined. This is because axial
volume sampling limits the resolution in this direction to the
Coregistration, sometimes called fusion, relies upon de-
width of each individual slice. Soft tissue contrast with CT
termining a transformation matrix that converts data from
is often poor, making it difficult to reliably contour the
one image set to the other. Image information can then be
borders of the prostate, especially at the base and the apex
overlaid to calculate and display information from both sets.
Defining this transformation matrix requires at least three
The ability of MRI to visualize soft tissue anatomy makes
data points, although the most successful coregistration
it an enticing choice as an imaging modality for prostate
methods use a much larger number of data points. Examples
brachytherapy dosimetry. Several authors have used MRI in
in prostate brachytherapy include using marker seeds (10),
this regard (31, 32). The MRI set is not restricted to axial
the urethral surface (33), and multiple seed locations (35).
acquisition, a particularly useful attribute for delineating the
There are pitfalls associated with coregistration of two
glandular borders at the troublesome apex and base. Critical
image sets. There can be changes in the patient position
structures such as the urethra and the neurovascular bundle
relative to the coordinates used to generate the transforma-
tion matrix, or changes in the relative positions between the
There are many problems associated with MRI dosimetry
coordinates themselves. For instance, using a urethra dis-
of the prostate. In addition to the same seed sorting prob-
tended by the presence of a catheter in one image set to
lems inherent to any cross-sectional image set, visualization
align an image set that had been generated without a cath-
of the seeds themselves is difficult. Because there is no
eter would likely produce errors. For the same reason,
signal from them, they image as low signal areas, making
extreme care must be exercised when aligning image sets
them difficult to distinguish from vessels, calcifications, and
based upon source locations from images produced at two
other structures with no signal. This is particularly difficult
widely different times after the implant. A similar argument
at the periphery and just outside the gland. While some
can be made against coregistering TRUS images taken
success has been achieved by choosing an imaging se-
before implant with the CT images taken after implant,
quence using bone windows with a narrow bandwidth (thus
unless sufficient time has passed for the postimplant edema
enhancing the artifact from the seeds), MRI does not image
sources as well as CT does. The acquisition process is
Distortion can also be a problem. A simple transforma-
certainly slower than CT, possibly contributing to motion
tion that results in scaling translation and rotation cannot
artifacts. Distortion of the image set may also be a problem
correct for a distorted data set. Fortunately, over the dis-
tances of concern in prostate brachytherapy, and with the
Although no reports have been published on the use of
equipment that is currently available, distortion of any sin-
TRUS for postimplant dosimetry, it has been used for re-
gle data set is usually minimal. Coregistration techniques
I. J. Radiation Oncology ● Biology ● Physics
that ignore distortion have thus far proved adequate for
thickness and spacing are commonly reported in the litera-
permanent prostate brachytherapy, because the distortion is
ture) (6, 10, 17, 18, 42–44).
minimal due to the small distances in prostate brachyther-
A catheter placed in the bladder and filled with contrast
can be used to localize the urethra and internal bladder wall.
A simple example of coregistration is the overlay of
However, the use of a catheter should be weighed against
isodose curves generated from plane film dosimetry on axial
the discomfort and potential morbidity of this procedure
CT images. Alignment is performed visually, sometimes
(especially if the CT scan is not performed in the immediate
aided by the placement of a gold marker seed placed at the
postimplant period when the patient already has an indwell-
apex of the gland. Transverse slices in the plane film coor-
dinate system are generated by the planning system and then
CT images are acquired using normal body-CT settings.
overlaid on the appropriate CT slice. Although this practice
If hardcopy films are to be used for digitization of seeds and
is common, it is fraught with uncertainties, and therefore is
prostate, an optimal window setting must be chosen that
of marginal value in permanent prostate brachytherapy. The
balances the ability to resolve seeds with the ability to
rapid changes in dose within relatively short distances make
delineate the prostate and adjacent structures of interest. The
it necessary to be as accurate as possible in determining the
geometry of the implant, and therefore the dosimetry, is
transformation matrix. This level of accuracy can be
derived directly from the CT images themselves. In some
achieved only with methods of determination that are quan-
CT scans, the images may contain distortions (such as
unequal x and y scaling), and it is important that means of
Roberson, Narayana, and colleagues have used marker
identifying and accounting for such scaling variations be in
seeds, as well as the urethral and rectal surfaces, to coreg-
ister the preimplant ultrasound and the postimplant CT scan
The TG-43 formalism is recommended for both the pre-
(10, 33). A similar technique in which the urethra and
and postimplant dosimetry (45–48). Due to the difficulties
bladder base are visually aligned to coregister postimplant
in using CT scans to determine seed orientation, the use of
CT and MRI image sets has recently been used by Amdur et
a point source approximation with anisotropy constant is
al. (36). A more rigorous method of coregistering image
recommended (49). Calculations should be performed using
sets based on the available source locations in each data set
a matrix with resolution limited to 2 mm or less (50) in an
has been outlined by Dubois et al. (35). This method has
effort to minimize the effects of the large dose gradients
been used to coregister postimplant CT and MRI data sets
inherent in a brachytherapy procedure.
and to fuse postimplant CT data sets to ultrasound image
The target is defined as the prostate (without margin) on
sets acquired to plan a second salvage implant (37).
the individual CT images. Care should be taken to distin-guish the prostate from the peri-prostatic tissue. Severalstudies have noted discrepancies in volume of prostate, as
determined by TRUS, MRI, and CT, reflecting the difficul-
At the present time, CT-based evaluation of the prostate
ties in differentiating the prostate from the periprostatic
implant appears to best satisfy the requirements of seed
musculature and venous plexus using CT (23, 33, 44, 51).
localization target and normal structure delineation and
Normal structures of interest that can be defined by using
seed-target registration. It is also readily available. Due to
CT include the urethra and the rectum (17, 18, 52, 53). For
possible seed migration or embolization (38–41), the num-
the urethra, the entire prostatic urethra should be defined.
ber of seeds implanted may not be the same as the number
This can be done through use of a central lumen point
of seeds present in the prostate at the time of the postimplant
identified on each slice, or by contouring the urethral wall
scan. Therefore, a better approximation of the number of
(52, 54). Catheterization is an accurate method for localiza-
seeds may be obtained by using plane radiographs. The
tion of the urethra within the prostate. If, however, the
recommended technique for performing CT-based dosime-
urethra cannot be visualized, an alternative is to identify, as
the urethral dose point, the geometric center of the prostate
The region to be imaged by CT should include the pros-
as imaged on successive CT slices (55). It must be recog-
tate, all the seeds within and around the prostate, and any
nized that doing this gives only an estimate of the urethral
critical structures for which the dose is to be reported. To
dose, and is valid only if peripheral seed-loading configu-
accomplish this, it is suggested that at minimum, a 2-cm
margin be added to the superior and inferior extent of the
For purposes of dosimetry, only the anterior rectal wall,
prostate. A reduced field of view that completely encom-
and not the entire rectum, is considered the structure of
passes the volumes and structures of interest, but offers a
interest. As with the urethra, several different methods may
finer resolution in the plane of the implant, should be used.
be used to define the rectal wall. These include the use of
This will reduce the error associated with seed localization
single points located along the anterior wall of the rectum,
contouring the outer anterior rectal wall for use with surface
Contiguous axial slices are recommended to reduce the
dosimetry or contouring the anterior rectal wall as a volume
chance of missing seeds between scans. The slice thickness
excluding the lumen (53, 56, 57). As most commercial
and spacing should be no greater than 5 mm (3-mm slice
planning systems are unable to define the dose to surfaces,
Prostate postimplant dosimetry ● S. NAG et al.
Table 2. Effect of timing on CT-based dosimetric evaluation
based on interseed spacing in an effort to eliminate theuncertainty introduced by CT-based prostate margin delin-
eation. It was proposed that this alternative would serve as
a more accurate estimation for target volume changes. How-
ever, the volumes estimated by this method were in reason-able agreement with those determined by contouring the
The optimal time to evaluate permanent prostate implant
dosimetry is controversial, and may differ by isotope (be-
cause of the difference in half-lives). Time-averagedweighting factors (58) and computer modeling (60–62) sug-gest that 103Pd and 125I implants would best be evaluated
contouring the anterior rectal wall as a volume represents a
after about 2 and 4 weeks, respectively. However, the do-
simetric compromise introduced by performing evaluation
It is possible for an individual seed to appear on multiple
of 103Pd implants at 1 month was demonstrated to be quite
CT slices. Although the frequency of this event may be
small (58). For various practical and logistical reasons,
reduced by using the larger (5 mm) slice spacing, it is not
many brachytherapists prefer to rely on early scanning (2, 3,
eliminated. Therefore, a seed-sorting computer program is
6, 18, 38, 59, 63). Many patients come from great distances
needed to eliminate this duplication or redundancy, and to
and may be unwilling to make return trips just for postop-
yield a final seed count consistent with the presumed num-
erative imaging studies. Additionally, early feedback can be
ber of seeds within the volume. As previously stated, plane
used to compensate an underdosed prostate (by reimplant-
radiographs are recommended in conjunction with CT-
ing or adding external beam) and to improve the implanta-
based dosimetry to aid seed sorting routines that require
tion technique. With early dosimetry, Willins and Wallner
prior knowledge of the number of seeds to be identified
estimated that coverage of the gland by at least 80% of the
from the larger set of seeds localized on CT. The “z” or
target isodose line was adequate (6, 63). These consider-
cranio-caudal coordinate of seeds identified on multiple CT
ations may outweigh the 10% underestimation of prostate
slices may be better defined by averaging over the CT
coverage that can be produced by early dosimetry (58).
coordinates of the different slices on which that seed has
Based on these considerations it can be stated that:
1. There is controversy and lack of consensus regarding the
ideal time to obtain postoperative dosimetry. The clinical
The degree of volumetric enlargement of the prostate
significance of obtaining dosimetry at different time in-
induced by the multiple needle punctures associated with
this procedure has been described. It is presumed that the
2. The most practical postoperative time interval for scan-
etiology of this volume increase is the trauma-associated
fluid accumulation and bleeding within the gland. Although
3. The most reproducible dosimetric results will be ob-
the percent of volume increase has been reported as ranging
tained if the scan is performed 1 month postimplant,
from 0 to 96%, mean values range from approximately 20%
although this may not be practical in all patients.
to 50% (5, 31, 33, 58–60) (Table 2). The broad range of
4. Until the ideal postoperative interval for scanning has
values is most likely related to a number of factors, which
been determined, each center should perform dosimetric
might include biological variation between patients, as well
evaluation of prostate implants at a consistent postoper-
as differences in experience and technique among brachy-
ative interval. This interval should be stated in the do-
therapists. There seems, however, to be better agreement on
simetry report. It should be kept in mind that dosimetry
the rate of resolution of this edema, with reported half-lives
obtained from CT scan in the immediate postimplant
period will underestimate prostate coverage by about
The magnitude dynamics and resolution of edema may
10%, compared to dosimetry obtained from CT scan
have obvious implications for the timing at which the dose-
volume relationship is described. There are few reports ofchanges in CT-based dosimetry in a serial fashion over time
Dosimetric evaluation and reporting
postimplant. In the first, Prestidge and colleagues (58) re-
Evaluation of postimplant dosimetry is typically carried
ported a mean maximum volume increase of 19%. This
out in three separate steps: (a) examination of isodose
resulted in a 10% underestimate of prostate coverage by the
distribution, (b) generation of the dose-volume histogram
prescribed dose on postoperative day 1 relative to day 180.
(DVH), and (c) determination of dose uniformity and dose
Waterman et al. (5) found a mean volume increase of
conformity indices. These three aspects of dosimetric eval-
52% on day 1 relative to preimplant, which resulted in a
uation provide complementary information for assessing the
mean decrease of approximately 10% in calculated dose
coverage. In this report, edema was initially calculated
A two-dimensional isodose distribution should be gener-
I. J. Radiation Oncology ● Biology ● Physics
Fig. 1. (a) Cumulative DVH of dose in percent of D
versus volume in percent of the target volume. (b) Differential
versus fractional volume in arbitrary scale.The full width at half maximum (FWHM)
ated on multiple slices throughout the prostate and in other
areas of concern. Outline of the prostate and any adjacent
100%, 90%, and 80% of the prostate, respectively).
critical structures as determined by tomographic imaging
should be superimposed on the isodose distribution. Such
tional volume of the prostate that receives 200%, 150%,
isodose plots offer the most direct assessment of dose cov-
100%, 90%, and 80% of the prescribed dose, respective-
erage, because the location of any underdosage in the pros-
tate can be evaluated based on supplemental clinical judg-
3. The total volume of the prostate (in cc) obtained from
ment. It is recommended that at least the following set of
isodose lines be generated as a percentage of the prescrip-
4. The number of days between implantation and the date
tion dose: 200%, 150%, 100%, 90%, 80%, and 50%.
of the imaging study used for dosimetric reconstruction.
Generation of the DVH of the prostate is recommended.
The most common format is the cumulative DVH, whichshows the percent volume (or total volume) of the prostate
All of the above volumetric parameters are obtainable from
that receives greater than or equal to a given dose. A less
a single compilation of the DVH. Of these, only D
commonly used representation, the differential dose-volume
been shown to correlate with PSA-based clinical outcome
histogram (DDVH), displays the relative volume of the
(11) and should be reported by all. However, in the research
prostate that receives a given dose (Fig. 1). The full width at
environment, a complete set of dosimetric data should be
half maximum (FWHM) of the DDVH is a measure of the
collected to facilitate future clinical correlation with respect
uniformity of the dose distribution. It is generated on the
to local control radiation toxicity and for comparison of
DDVH by taking the peak volume value, dividing by two,
results between various institutions.
and drawing a horizontal line on the graph. The dose where
A number of dose conformity quantifiers exist in the
the line first hits the rising curve is subtracted from the dose
literature for prostate brachytherapy (64, 69, 70). Of these,
represented by the last intersection of the line and the falling
the target volume ratio (TVR) is traditionally defined as the
curve, giving the FWHM. A larger value implies a wider
ratio of the reference dose volume to the target volume. The
range of doses or a less uniform dose distribution. A smaller
concept of TVR is similar to the historical matched periph-
value thus reflects a more uniform dose distribution. The
eral dose and has the same limitation of not addressing the
geometrical relationship between the target volume and the
Typically, the DDVH peaks at a dose that is higher than
reference dose volume: a geometrical miss will not be
the prescription dose. The spread of the peak is a useful
reflected in the TVR value. It is possible to perform an
indicator of dose homogeneity (18, 64, 65). A smaller
implant with a TVR Ͼ 1.0 (seemingly good), where very
spread indicates greater dose uniformity. It is recommended
little dose was actually delivered to the prostate (bad) if
that a grid size of 2 mm or smaller be used to ensure
most of the sources were outside the prostate. A modified
adequate resolution of the reported parameters in the dosi-
TVR (TVR2), as described by Bice and Prestidge (43),
metric calculation (17, 66–68).
takes into account the volume and the location encompassed
It is recommended that the following be reported to allow
by the reference isodose surface. TVR2 is defined as the
adequate evaluation of postimplant dosimetry and to allow
reference dose volume divided by the volume of the target
that receives the reference dose or greater. While this quan-
Prostate postimplant dosimetry ● S. NAG et al.
tifier still has some flaws, TVR2 has the advantage of
Ͻ 140 Gy, compared to 92% for those with a
including the spatial relationship between the target and the
dose, but is dependent upon who and how the target is
Treatment-related morbidity has also been correlated
drawn. Because the clinical target volume in prostate
with postimplant dosimetry findings. Wallner et al. (52)
brachytherapy is not yet fully understood, this dose confor-
analyzed 45 patients treated with 125I implantation who had
mity parameter was not found to be a useful enough param-
CT-based dosimetry performed 2–4 h after implantation and
eter to receive a strong endorsement or a recommendation
related these findings to urinary and rectal morbidity. He
from the panel. While it may be of value in assessing future
found that in patients who developed RTOG grade 0–1
clinical outcomes, it is not required of the community
urinary morbidity, an average of 10 mm of urethra was
irradiated to doses Ͼ 400 Gy (pre-TG43) compared to 20
Calculation and reporting of dose to the prostatic urethra
mm for patients experiencing Grade 2–3 morbidity (p ϭ
are important components of dosimetric evaluation. Dose to
0.07). He concluded that both the dose and length of urethra
the urethra may be represented in a number of ways. If the
irradiated were related to urinary morbidity. Similarly,
urethra is adequately visualized (e.g., by catheterization) in
when examining rectal morbidity, he found that in patients
postimplant imaging, a DVH or dose-surface histogram
developing RTOG Grade 1–2 rectal morbidity an average of
(DSH) can be generated in addition to point dose calculation
17 mm2 of rectal wall was irradiated to doses Ͼ 100 Gy,
at the center of the urethra on each axial slice. Less reliably,
compared to 11 mm2 for patients experiencing no rectal
the geometric center of the prostate may be used as a
surrogate for the location of the urethra, particularly for the
Desai et al. (54) analyzed acute urinary morbidity in 117
peripheral loaded implants (55). The urethral dose through-
patients treated with 125I implants by correlating urinary
out the prostate should be examined on multiple sections.
symptoms as measured by the international prostate symp-
The length of urethra receiving Ͼ 200% of the prescribed
tom score with findings from CT-based dosimetry per-
dose should be recorded to allow correlation with urethral
formed 1 month after implantation. She found that the
highest symptom score in each patient correlated with the
Similarly, dose to the anterior rectal wall is an important
following dose descriptions of the prostate: D
component of postimplant evaluation. Rectal dose may be
represented in a DSH or DVH within an annulus that
approximates the anterior rectal wall (56). Alternatively, for
doses delivered to 5 cm2 of urethra, as measured by DSH.
simplicity, point dose sampling along the anterior rectal
The conclusion of this analysis was that attempts at reduc-
wall may be used. Again, the rectal dose should be recorded
ing urethral doses can translate into reduced urinary symp-
toms, and that trials of prostate dose escalation may be
It is recognized that detailed DVH analysis may be very
limited by the acute urinary symptoms (54).
labor intensive and may not be supported by all treatmentplanning systems at present. Therefore, it may not be prac-
DISCUSSION
tical to report all of the above dosimetric parameters in thecommunity setting. However, it is recommended that at a
Postimplant dosimetry of the prostate is a constantly
minimum, postimplant dosimetry be performed and the D
evolving dynamic field. The above recommendations rep-
reported at all centers, and that all the other parameters be
resent the current consensus opinion of the ABS. Because of
additionally obtained in a research environment.
the current paucity of published data, there are areas ofcontroversy that cannot be resolved. For example, the ideal
time for obtaining the postimplant dosimetry or an exact
The data collected from dosimetric analysis is relevant in
dose/volume recommendation to the urethra or rectum can-
that it has been shown to correlate with treatment outcomes.
not currently be identified. The panel identified a number of
Historically, measures of implant quality of retropubic pros-
other parameters that should be considered for further de-
tate brachytherapy have been related to disease control
velopment and refinement of the dosimetric process.
Currently, dosimetric analysis is performed after the im-
Stock et al. analyzed the results of CT-based postimplant
plant has been completed. This does not provide a mecha-
dosimetry (using TG43 guidelines) performed 1 month after
nism for correction if suboptimal dose distribution is ob-
implantation in 134 patients treated with 125I implants for
tained. Ideally, one should strive for on-line real-time
T1 to T2 prostate cancer over a 6-year period. This study
intraoperative dosimetry to allow for adjustment in seed
correlated dosimetric findings with PSA control and nega-
placement to achieve the intended dose. Current ultrasound
technology must be improved to localize the individual seed
100–119.9 Gy, 120–139.9 Gy, 140–159.9 Gy, and Ն 160
position within the prostate, and isodose calculations must
Gy were associated with improved freedom from PSA fail-
be rapidly performed on-line and updated as subsequent
ure rates of 53%, 82%, 80%, 95%, and 89%, respectively
seeds are implanted. Correlation of the resultant implant
(p ϭ 0.02) at 4 years. A dose cutoff point was found at 140
dose distribution to the clinical outcome has yet to be
Gy, with PSA control rates of 68% for those patients re-
I. J. Radiation Oncology ● Biology ● Physics
The dose distribution in a prostate implant is very inho-
complex to be practical for the practicing community radi-
mogeneous. The degree of dose heterogeneity varies from
ation oncologist, and may be more relevant for the larger
implant to implant. The tumor control probability (TCP)
brachytherapy centers planning to compare their outcome
depends on the degree of heterogeneity in addition to the
results. This differentiation has been mentioned in the rel-
prescribed dose (74). For example, in two implants with the
same D , the dose may be much higher (or lower) in some
regions of one than in similar regions of the other. The
implant with the more heterogeneous dose may have agreater TCP, because parts of the tumor will receive a dose
The ABS recommends that postimplant dosimetry should be
that is much higher than the prescribed dose. The therapeu-
performed on all patients undergoing permanent prostate
tic advantage and tradeoff of dose heterogeneity are not yet
brachytherapy for optimal patient care. At present, CT-based
adequately documented for the purpose of clinical correla-
dosimetry is recommended based on availability, cost and the
ability to image the prostate as well as the seeds. Additional
Another factor to be considered is the presence of large
plane radiographs should be obtained to verify the seed count.
prostate calcifications that can affect the dose delivered. The
Until the ideal postoperative interval for CT scanning has been
higher atomic number of calcium (z ϭ 20) compared to that
determined, each center should perform dosimetric evaluation
of prostatic tissue (z ϭ 7.6) leads to a greater absorbed dose
of prostate implants at a consistent postoperative interval. This
increased attenuation and increased dose deposition at the
interval should be reported. Isodose displays should be ob-
calcium/soft tissue interface. Interseed effects may also
tained at 50%, 80%, 90%, 100%, 150%, and 200% of the
adversely affect the dose distribution, because the seeds,
prescription dose and displayed on multiple cross-sectional
being denser than tissue, will absorb some of the radiation
images of the prostate. A DVH of the prostate should be
from other seeds (75, 76). The actual effect of these heter-
ogeneities on the dose distribution needs further investiga-
rectal, and urethral doses should be reported and ultimately
Finally, these recommendations are intended to be advi-
correlated with clinical outcome at larger centers. On-line,
sory in nature; the responsibility for the medical decisions
real-time dosimetry, the effects of dose heterogeneity, and the
ultimately rests with the treating physician who has to
effects of tissue heterogeneity need further investigation. These
consider the cost-benefit ratio. We also recognize that some
recommendations should be a practical guide for performing
of the recommendations given in this report may be too
postimplant dosimetry for permanent prostate brachytherapy. REFERENCES
1. Prete JJ, Prestidge BR, Bice WS, et al. A survey of physics
ment deviations from pre-planned positions in ultrasound
and dosimetry practice of permanent prostate brachytherapy in
guided prostate implants. Radiother Oncol 1994;32:268–270.
the United States. Int J Radiat Oncol Biol Phys 1998;40:1001–
9. Narayana V, Roberson PL, Winfield RJ, et al. Optimal place-
ment of radioisotopes for permanent prostate implants. Radi-
2. Nag S, Baird M, Blasko J, et al. American Brachytherapy
ology 1996;199:457–460.
Society (ABS) survey of current clinical practice for perma-
10. Roberson PL, Narayana V, McShan DL, et al. Source place-
nent brachytherapy of prostate cancer. J Brachyther Int 1997;
ment error for permanent implant of the prostate. Med Phys
3. Nag S, Beyer D, Friedland J, et al. American Brachytherapy
11. Stock RG, Stone N, Tabert A, et al. A dose-response study for
Society (ABS) recommendations for transperineal permanent
I-125 prostate implants. Int J Radiat Oncol Biol Phys 1998;
brachytherapy of prostate cancer. Int J Radiat Oncol Biol
12. Lerner SE, Blute ML, Zincke H. Critical evaluation of salvage
surgery for radiorecurrent/resistant prostate cancer. J Urol
4. Yu Y, Waterman FM, Suntharalingam N, et al. Limitations of
the minimum peripheral dose as a parameter for dose speci-
13. Stock RG, Stone NN. Salvage brachytherapy for recurrent
fication in permanent 125I prostate implants. Int J Radiat
prostate cancer following radiation therapy. In: Zelefsky,
Oncol Biol Phys 1996;34:717–725.
Greco C, editors. Radiotherapy of prostate cancer. United
5. Waterman FM, Yue N, Corn BW, et al. Edema associated
Kingdom: Harwood Academic. In press.
with I-125 or Pd-103 prostate brachytherapy and its impact on
14. Grado GL, Collins JM, Kriegshauser JS, et al. Salvage brachy-
post-implant dosimetry: An analysis based on serial CT ac-
therapy for localized prostate cancer after radiotherapy failure.
quisition. Int J Radiat Oncol Biol Phys 1998;41:1069–1077. Urology 1999;53:2–10.
6. Willins J, Wallner K. CT-based dosimetry for transperineal
15. Prestidge BR, Bice WS, Prete JJ, et al. A dose-volume anal-
I-125 prostate brachytherapy. Int J Radiat Oncol Biol Phys
ysis of permanent transperineal prostate brachytherapy. (Ab-
str.) Int J Radiat Oncol Biol Phys 1997;39:289.
7. Bice WS, Prestidge BR, Grimm PD, et al. Centralized multi-
16. Sharkey J, Chovnick SD, Behar RJ, et al. Outpatient ultra-
institutional post-implant analysis for interstitial prostate
sound-guided palladium-103 brachytherapy for localized ad-
brachytherapy. Int J Radiat Oncol Biol Phys 1998;41:921–
enocarcinoma of the prostate: A preliminary report of 434
patients. Urology 1998;51:796–803.
8. Dawson JE, Wu T, Roy T, et al. Dose effects of seed place-
17. Stone NN, Stock RG, DeWyngaert JK, et al. Prostate brachy-
Prostate postimplant dosimetry ● S. NAG et al.
therapy: Improvements in prostate volume measurements and
38. Nag S, Scaperoth DD, Badalament R, et al. Transperineal
dose distribution using interactive ultrasound guided implan-
palladium-103 prostate brachytherapy: Analysis of morbidity
tation and three-dimensional dosimetry. Radiat Oncol Invest
and seed migration Urology 1995;45:87–92.
39. Tapen EM, Blasko JC, Grimm PD, et al. Reduction of radio-
18. Roy JN, Wallner KE, Harrington PJ, et al. A CT-based eval-
active seed embolization to the lung following prostate
uation method for permanent implants: Application to pros-
brachytherapy. Int J Radiat Oncol Biol Phys 1998;42:1063–
tate. Int J Radiat Oncol Biol Phys 1993;26:163–169.
19. Altschuler MD, Findlay PA, Epperson RD. Rapid accurate
40. Steinfeld AD, Donahue BR, Plaine L. Pulmonary emboliza-
three-dimensional location of multiple seeds in implant radio-
tion of iodine-125 seeds following prostate implantation.
therapy treatment planning. Phys Med Biol 1983;28:1305–
41. Nag S, Vivekanandam S, Martinez-Monge R. Pulmonary em-
20. Siddon RL, Chin LM, Two-film brachytherapy reconstruction
bolization of permanently implanted radioactive palladium-
algorithm. Med Phys 1985;12:77–83.
103 seeds for carcinoma of the prostate. Int J Radiat Oncol
21. Metz C, Fencil LE. Determination of three dimensional struc-
Biol Phys 1997;39:667–670.
ture in biplane radiography with prior knowledge of the rela-
42. Stock RG, Stone NN, Wesson MF, et al. A modified technique
tionship between the two views: Theory. Med Phys 1989;16:
transperineal prostate implantation. Int J Radiat Oncol Biol
22. Hughes HA. Accuaracy of foreign body localization from tube
Phys 1995;32:219–225.
shift radiographs. Br J Radiol 1956;29:116–118.
43. Bice WS, Prestidge BR. A review of postimplant quality
23. Rosen II, Khan KM, Lane RG, et al. The effect of geometric
assessment in permanent transperineal interstitial prostate
errors in the reconstruction of iridium-192 seed implants. Med
brachytherapy. J Brachyther Int 1997;13:297–313. Phys 1982;9:220–223.
44. Badiozamani KR, Wallner K, Cavanagh W, et al. Compara-
24. Fitzgerald LT, Mauderli W. Analysis of errors in three-dimen-
bility of CT-based and TRUS-based prostate volumes. Int J
sional reconstruction of radium implants from stereo radio-
Radiat Oncol Biol Phys 1999;43:375–378.
graphs. Radiology 1975;115:455–458.
45. Nath R, Anderson LL, Luxton G, et al. Dosimetry of intersti-
25. Amols HI. Rosen II. A three-film technique for reconstruction
tial brachytherapy sources: Recommendations of the AAPM
of radioactive seed implants Med Phys 1981;8:210–214.
Radiation Committee Task Group No. 43. Med Phys 1995;22:
26. Biggs PJ, Kelley DM. Geometric reconstruction of seed im-
plants using a three-film technique. Med Phys 1983;10:701–
46. Luse RW, Blasko J, Grimm P. A method for implementing the
American Association of Physicists in Medicine Task
27. Altschuler MD, Kassaee A. Automatic matching of corre-
Group-43 dosimetry recommendations for 125I transperineal
sponding seed images of three simulator radigraphs to allow
prostate seed implants on commercial treatment planning sys-
3-D triangulation of implanted seeds. Phys Med Biol 1997;42:
tems. Int J Radiat Oncol Biol Phys 1997;37:737–741.
47. Bice WS, Prestidge BR, Prete JJ, et al. Clinical impact of
28. Brinkman DH. Kline RW. Automated seed localization from
implementing the recommendations of AAPM Task Group 43
CT data sets of the prostate. Med Phys 1998;25:1667–1672.
permanent prostate brachytherapy using 125I. Int J Radiat
29. Bice WS, Dubois DF, Prete JJ, et al. Source localization from
Oncol Biol Phys 1998;40:1237–1241.
axial image sets by iterative relaxation of the nearest neighbor
48. Williamson J, Coursey B, DeWerd L, et al. Dosimetric pre-
criterion. Med Phys Submitted.
requisites for routine clinical use of new low energy photon
30. Dubois DF, Prestidge BR, Hotchkiss LA, et al. Intraobserver
interstitial brachytherapy sources. Med Phys 1998;25:2269–
and interobserver variability of MR imaging and CT-derived
prostate volumes after transperineal interstitial permanent
49. Yu Y, Anderson LL, Li Z, et al. Permanent prostate seed
prostate brachytherapy. Radiology 1998;207:785–789.
implant brachytherapy: Report of the American Association of
31. Moerland MA, Wijrdeman HK, Beersma R, et al. Evaluation
Physicists in Medicine Task Group No. 64. Med Phys. In
of permanent I-125 prostate implants using radiography and
magnetic resonance imaging. Int J Radiat Oncol Biol Phys
50. Anderson LL. Brachytherapy planning and evaluation. En-docurie Hyperther Oncol 1991;7:139–146.
32. Dubois DF, Prestidge BR, Hotchkiss LA, et al. Source local-
51. Roach M, Faillace-Akazawa P, Malfatti C, et al. Prostate
ization following permanent transperineal prostate interstitial
volumes defined by magnetic resonance imaging and comput-
brachytherapy using magnetic resonance imaging. Int J Radiat
erized tomographic scans for three-dimensional conformal
Oncol Biol Phys 1997;39:1037–1041.
radiotherapy. Int J Radiat Oncol Biol Phys 1996;35:1011–
33. Narayana V, Roberson PL, Pu AT, et al. Impact of differences
in ultrasound and computed tomography volumes on treat-
52. Wallner K, Roy J, Harrison L. Dosimetry guidelines to min-
ment planning of permanent prostate implants. Int J Radiat
imize urethral and rectal morbidity following transperineal
Oncol Biol Phys 1997;37:1181–1185.
I-125 prostate brachytherapy. Int J Radiat Oncol Biol Phys
34. Narayana V, Roberson PL, Winfield RJ, et al. Impact of
ultrasound and computed tomography prostate volume regis-
53. DeWyngaert JK, Wesson MF. Treatment planning consider-
tration on evaluation of permanent prostate implants. Int J
ations of ultrasound guided I-125 prostate implants. Int JRadiat Oncol Biol Phys 1997;39:341–346. Radiat Oncol Biol Phys 1991;21(Suppl. 1):160.
35. Dubois DF, Bice WS, Prestidge BR, et al. CT and MRI
54. Desai J, Stock RG, Stone NN, et al. Acute urinary morbidity
derived source localization error in a custom prostate phantom
following iodine-125 interstitial implantation of the prostate
using automated image coregistration. Med Phys. In press.
gland. Radiat Oncol Invest 1998;6:135–141.
36. Amdur R, Gladstone D, Leopold K, et al. Prostate seed im-
55. Waterman FM, Dicker AP. Determination of the urethral dose
plant quality assessment using MR and CT image fusion. Int
in prostate brachytherapy when the urethra is not visualized in
J Radiat Oncol Biol Phys 1999;43:67–72.
the post-implant CT scan. (Abstr.) Med Phys. In press.
37. Bice WS, Freeman JE, Russell J, et al. Coregistration of
56. Lu Y, Li S, Spelbring D, et al. Dose-surface histograms as
post-implant ultrasound and CT image sets in permanent pros-
treatment planning tool for prostate conformal therapy. Med
tate brachytherapy. Int J Radiat Oncol Biol Phys. Submitted. Phys 1995;22:279–284.
I. J. Radiation Oncology ● Biology ● Physics
57. Zelefsky MJ, Happersett L, Leibel S, et al. The effect of
66. Anderson L. Brachytherapy planning and evaluation. Endocu-
treatment positioning on normal tissue dose in patients with
rie Hypertherm Oncol 1991;7:139–146.
prostate cancer treated with three-dimensional conformal ra-
67. Paul J, Philip P, Brandenburg R, et al. Histograms in brachy-
diotherapy. Int J Radiat Oncol Biol Phys 1997;37:13–19.
therapy. Endocurie Hypertherm Oncol 1991;7:13–26.
58. Prestidge BR, Bice WS, Kiefer EJ, et al. Timing of computed
68. Waterman F, Strubler K. Absorbed dose determination for
tomography-based postimplant assessment following perma-
interstitial 125I boost therapy. Med Phys 1983;10:155–158.
nent transperineal prostate brachytherapy. Int J Radiat Oncol
69. van’t Riet A, Mak AC, Moerland MA, et al. A conformation
Biol Phys 1998;40:1111–1115.
number to quantify the degree of conformality in brachyther-
59. Merrick GS, Butler WM, Dorsey AT, et al. Influence of timing
apy and external beam irradiation: Application to the prostate.
on the dosimetric analysis of transperineal ultrasound-guided
Int J Radiat Oncol Biol Phys 1997;37:731–736.
prostatic conformal brachytherapy. Radiat Oncol Invest 1998;
70. Saw CB, Suntharalingam N. Quantitative assessment of inter-
stitial implants. Int J Radiat Oncol Biol Phys 1991;20:135–
60. Yue N, Nath R, Chen Z, et al. Optimum timing for CT-based
dose evaluation of I-125 and Pd-103 prostate seed implants.
71. Zelefsky MJ, Whitmore WF Jr. Long-term results of retropu-
(Abstr.) Int J Radiat Oncol Biol Phys 1998;42:134.
bic permanent 125iodine implantation of the prostate for clin-
61. Yue N, Dicker AP, Corn BW, et al. A dynamic model for the
ically localized prostatic cancer. J Urol 1997;158:23–29.
estimation of optimum timing of computed tomography scan
72. Nath R, Roberts K, Ng M, et al. Correlation of medical
for dose evaluation of 125I or 103Pd seed implant of prostate.
dosimetry quality indicators to the local tumor control in
Int J Radiat Oncol Biol Phys 1999;43:447–454.
patients with prostate cancer treated with iodine-125 intersti-
62. Moerland MA. The effect of edema on post-implant dosimetry
tial implants. Med Phys 1998;25:2293–2307.
of permanent iodine-125 prostate implants: A simulation
73. Fuks Z, Leibel SA, Wallner KE, et al. The effect of local
study. J Brachyther Int 1998;14:225–231.
control on metastatic dissemination in carcinoma of the pros-
63. Willins J, Wallner K. Time-dependent changes in CT-based
tate: Long-term results in patients treated with 125I implanta-
dosimetry of I-125 prostate brachytherapy. Radiat Oncol In-
tion. Int J Radiat Oncol Biol Phys 1991;21:537–547. vest 1998;6:157–160.
74. Ling CC, Roy J, Sahoo N, et al. Quantifying the effect of dose
64. Yu Y. A non-divergent specification of the mean treatment
inhomogeneity in brachytherapy: Application to permanent
dose in interstitial brachytherapy. Med Phys 1996;23:905–
prostatic implant with 125I seeds. Int J Radiat Oncol Biol Phys
65. van’t Riet A, Te Loo HJ, Ypma AF, et al. Ultrasonically
75. Burns G, Raeside D. The accuracy of single-seed dose super-
guided transperineal seed implantation of the prostate: Mod-
position of I-125 implants. Med Phys 1989;16:627–631.
ification of the technique and qualitative assessment of im-
76. Meigooni A, Meli J, Nath R. Interseed effects on dose for 125I
plants. Int J Radiat Oncol Biol Phys 1992;24:555–558.
brachytherapy implants. Med Phys 1992;19:385–390.
The Quarterly Newsletter for the UNC Center for Maternal & Infant Health Winter 2005 FROM THE DIRECTOR’S DESK Welcome to the Winter 2005 edition of CenterNews. We appreciate the opportunity to share medical news and information with you. Assuch, we are pleased to announce that our website www.mombaby.org has received a new look for the New Year. The site has been reorgan-ize
Palestine's economy is like a coiled spring, says British financier - Business News, Bu. Page 1 of 3 Yasmin Alibhai-Brown : Don't Israel's nuclear weapons count? Palestine's economy is like a coiled spring, says British financier Investment conference backed by Tony Blair told that political progress could spark rapid growth SPONSORED LINKS: Ads by Google QROPS Expert Advice Guide Exp
 Int. J. Radiation Oncology Biol. Phys., Vol. 46, No. 1, pp. 221–230, 2000
Copyright 2000 Elsevier Science Inc.
Int. J. Radiation Oncology Biol. Phys., Vol. 46, No. 1, pp. 221–230, 2000
Copyright 2000 Elsevier Science Inc.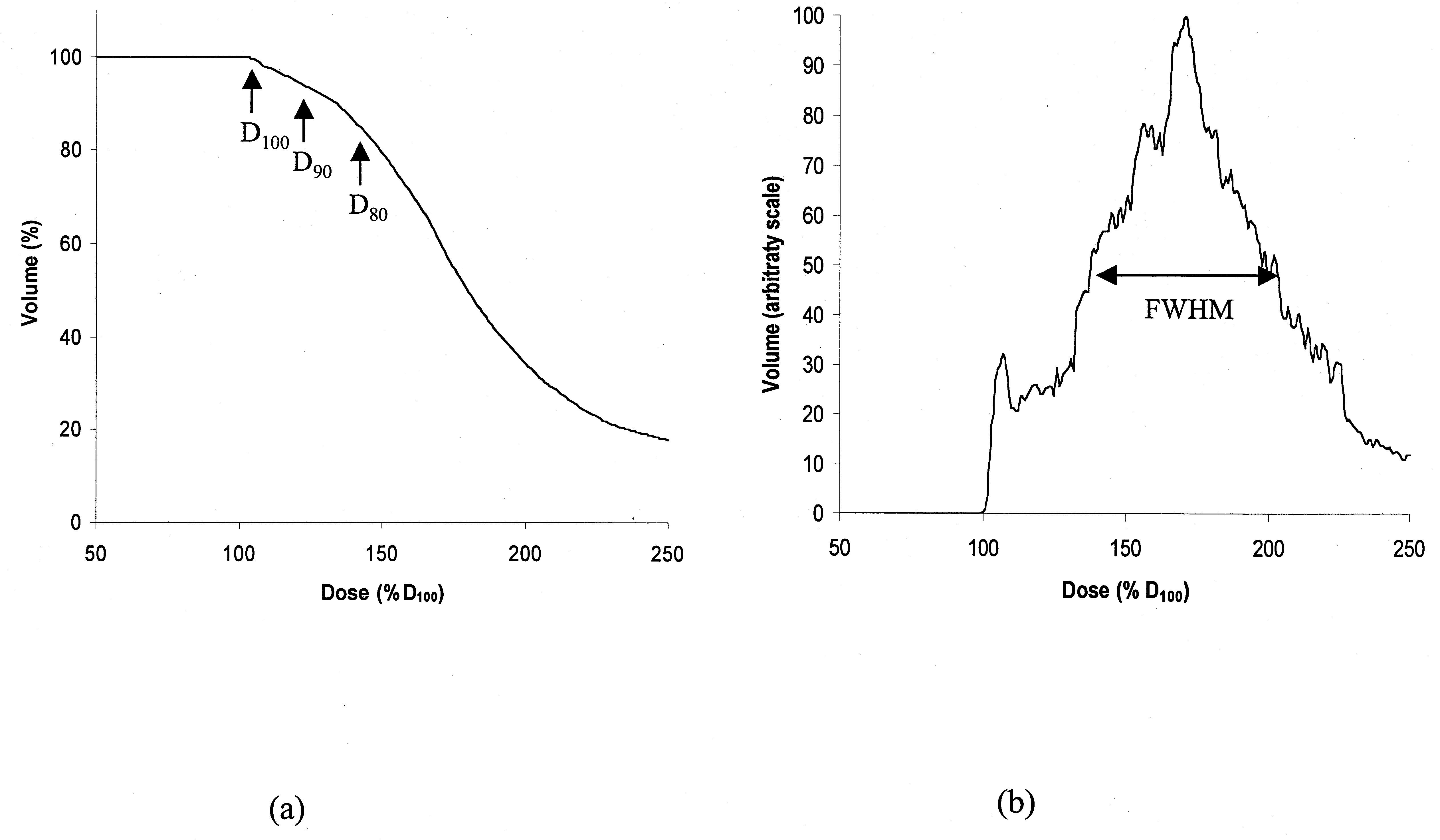 I. J. Radiation Oncology ● Biology ● Physics
Fig. 1. (a) Cumulative DVH of dose in percent of D
versus volume in percent of the target volume. (b) Differential
versus fractional volume in arbitrary scale.The full width at half maximum (FWHM)
ated on multiple slices throughout the prostate and in other
areas of concern. Outline of the prostate and any adjacent
100%, 90%, and 80% of the prostate, respectively).
I. J. Radiation Oncology ● Biology ● Physics
Fig. 1. (a) Cumulative DVH of dose in percent of D
versus volume in percent of the target volume. (b) Differential
versus fractional volume in arbitrary scale.The full width at half maximum (FWHM)
ated on multiple slices throughout the prostate and in other
areas of concern. Outline of the prostate and any adjacent
100%, 90%, and 80% of the prostate, respectively).