Overview of the Management of Atrial Fibrillation: What is the
PETER R. KOWEY, M.D., GAN-XIN YAN, M.D., PH.D., TARA L. DIMINO, M.D.,
From the Cardiovascular Division, Lankenau Hospital and Medical Research Center, and the Main Line Health Heart Center,
Wynnewood, Pennsylvania, USA; and the Department of Medicine, Jefferson Medical College of Thomas Jefferson University,
Management of Atrial Fibrillation. There are three fundamental approaches to the management of atrial fibrillation (AF): rate control, rhythm control, and anticoagulation. Selecting a course of treatment requires a thorough knowledge of these therapeutic alternatives. This article explores treatment options, including the relative benefits of rate control versus rhythm control, which are complicated by the lack of highly effective and safe antiarrhythmic drugs. Anticoagulation is also an important issue in AF man- agement, and warfarin effectively reduces the incidence of thromboembolic events in AF patients. The use of warfarin, however, presents its own complications. We conclude that individualization of therapy is paramount when treating AF. (J Cardiovasc Electrophysiol, Vol. 14, pp. S275-S280, December 2003, Suppl.) sinus arrhythmia, antiarrhythmic drugs, anticoagulants, atrial fibrillation, left ventricular dysfunctionIntroduction
AV nodal conduction, some rate control medication is nec-essary. Which drug is used and how it is delivered depends
Atrial fibrillation (AF) is a complicated disease state that
on several factors, including the drug’s pharmacologic pro-
requires a multifaceted management approach. It is not an
file, the urgency of the clinical situation, the patient’s clinical
exaggeration to say that this disease requires as much clin-
stability, and concomitant drug therapy and medical condi-
ical skill in management as any disorder that doctors treat.
tions.1,2 In general, rapidly acting calcium channel blockers
On one hand, we have learned that AF need not be treated
or beta-blockers are administered intravenously when a clin-
aggressively in many patients, but we also know that AF fre-
ical effect is needed quickly. It is important to note that only
quently is complicated by disabling stroke, an outcome worse
a minority of patients who develop AF have so much hemo-
than death for most patients who experience this devastating
dynamic compromise that intravenous administration of AV
and avoidable complication of the disease. Thus, as in no
nodal-blocking agents is necessary. In the majority, a short-
other condition, individualization of therapy is paramount,
acting oral beta-blocker or calcium channel blocker, with a
while still adhering, as best we can, to basic treatment dic-
short time to effect, may suffice, with longer-acting oral con-
tums derived from well-designed and well-executed clinical
geners reserved for long-term clinical use. Weaker AV nodal
blockers, such as digitalis, are reserved as adjuvant therapy
In this article, we consider the three major components
for patients whose AV nodes are diseased, when single-drug
of AF treatment: rate control, rhythm control, and antico-
treatment does not suffice, or for management of heart fail-
agulation. Because other articles in this issue of the Journal
ure.3-6 The adequacy of rate control is difficult to define, but
review specific therapies, we confine this discussion to the
heart rates of <80 beats/min at rest with attainment of <90%
broad categories, highlighting treatment options and the trial
of the maximum predicted heart rate with maximal exercise
evidence to support them. For most of this discussion, atrial
would be considered acceptable. Alternatively, criteria have
flutter will not be discussed separately unless there are spe-
been applied based on control of rate during a range of activ-
cific data pertaining to that arrhythmia that are not applicable
ities of daily living. It is critical, however, that optimization
of heart rate be judged with the patient at rest and then duringexertion, because the rate control effect of agents such as dig-
Rate Control
italis may be overcome by catecholamines, rendering the pa-tient uncontrolled during a significant portion of her/his daily
The first step in the treatment of AF generally is control of
routine.6,7 In those rare cases where conventional AV nodal-
the ventricular response rate. In elderly patients, especially
blocking agents are ineffective, such as in very ill patients,
those with conduction disease, rates may be well controlled
amiodarone may be useful because the drug’s earliest effect,
at the onset of AF, but for the majority of patients with intact
when administered intravenously, is negative dromotropismvia its noncompetitive beta-adrenergic and calcium channel-blocking effects.6 Careful rate control is paramount no mat-ter which agent is used, because high heart rates over time
Supported in part by the Rose and Adolph Levis Foundation, Haverford,Pennsylvania.
may cause severe symptoms as well as profound left ventric-ular dysfunction in some individuals.8,9 This is part of the
Address for correspondence: Peter R. Kowey, M.D., Main Line Health Heart
rationale for considering AV nodal ablation and permanent
Center, Lankenau Medical Office Building, Suite 558, 100 Lancaster Av-
pacemaker implantation in select patients who also may be
enue, Wynnewood, PA 19096. E-mail: prkowey@pol.net
suffering from severe symptoms caused by the rapidity and
irregularity of their arrhythmia.8 The relative benefits of rate
Journal of Cardiovascular Electrophysiology Vol. 14, No. 12, Supplement, December 2003
Pharmacologic conversion, although less effective, has the
potential of better patient acceptance and wider applicabil-ity. It is important to note that, in general, drugs are moreefficacious for converting AF of shorter than longer dura-tion. In fact, very few drugs have been systematically studiedand approved for this indication. Class IA and IC drugs havebeen used intravenously and orally with good reported suc-cess. The Class IC drugs appear to be effective and safe fortermination of AF of relatively recent onset in patients withnormal or nearly normal hearts, and they can be used eitherorally or parenterally.20-22 However, the drugs approved forthis indication are intravenous ibutilide and oral dofetilide,both Class III antiarrhythmic drugs. Ibutilide has no oral con-gener and thus is limited to acute therapy only. It appears towork better in patients with arrhythmias of relatively recentonset and has greater efficacy in atrial flutter.23,24 Its prin-cipal liability is torsades de pointes, which occurs in 2% to4% of patients and is more likely in women, the elderly, andpatients with left ventricular dysfunction.25-27 Dofetilide wasapproved for this indication based on its record of effective-ness in patients hospitalized for oral drug loading. Conversionto SR occurs in 30% of patients with persistent AF comparedwith a placebo conversion rate of about 1% to 3%.28 As with
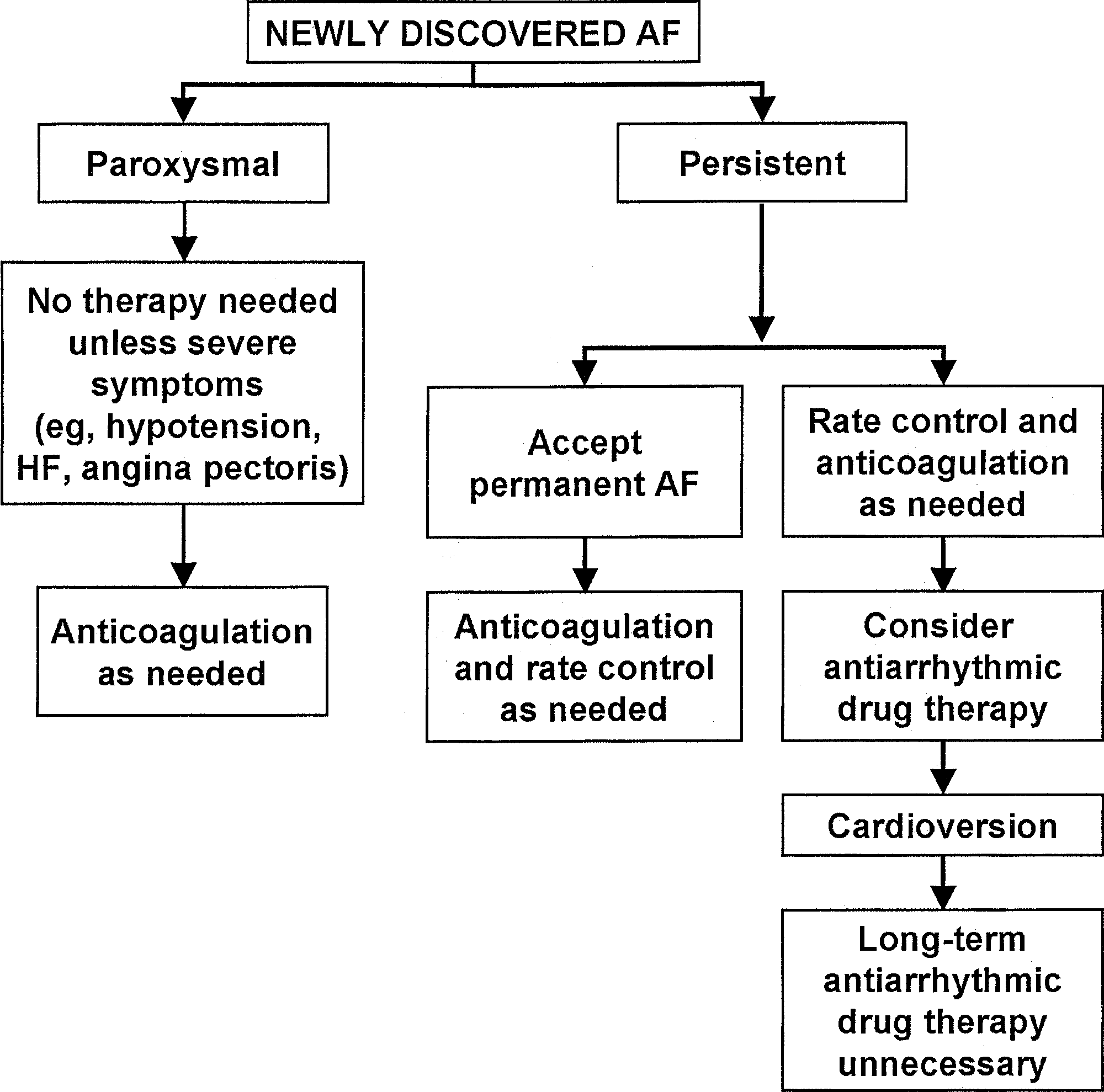
Figure 1. An approach to the management of “new” atrial fibrillation, as
ibutilide, dofetilide’s principal liability is torsades de pointes,
previously published in the ACC/AHA/ESC guidelines.10 (Reproduced with
which fortunately happens early in dosing while the patient
permission from Fuster V, Ryden LE, Asinger RW, et al.; American College
is under observation.25,27,29
of Cardiology/American Heart Association Task Force on Practice Guide-
Other drugs have been used for acute conversion of AF
lines; European Society of Cardiology Committee for Practice Guidelinesand Policy Conferences (Committee to Develop Guidelines for the Manage-
without convincing demonstration of effectiveness. Amio-
ment of Patients with Atrial Fibrillation); North American Society of Pac-
darone has gained popularity for this indication. Although
ing and Electrophysiology: ACC/AHA/ESC guidelines for the management
many previous studies were unconvincing as to amiodarone’s
of patients with atrial fibrillation: Executive summary. Circulation 2001;
efficacy for this indication,30 more recent data have sug-
gested that infusion of high doses for several hours mightbe useful.31 Spontaneous conversions in this populationoccur with such variable frequency that carefully done,
control versus rhythm control will be considered in a subse-
large, placebo-controlled trials are essential before any con-
clusions can be reached about the efficacy and safety ofdrugs for this indication. Amiodarone’s peculiar pharmacoki-
Rhythm Control
netic profile makes such studies difficult to execute and tointerpret.
The other broad strategy in AF management is mainte-
Proper anticoagulation prior to and following cardiover-
nance of sinus rhythm (SR) (Fig. 1).10 This approach has two
sion is a key item in its safe implementation. Fortunately,
parts: restoration of SR for patients whose AF is persistent,
we now have good data on which to base firm recommenda-
and chronic treatment to prevent AF recurrence. Conversion
tions about the proper use of anticoagulant therapy to prevent
of AF to SR can be accomplished electrically or pharma-
stroke and other thromboembolic events.30 These recommen-
cologically. Electrical conversion is well established, highly
dations will be presented in the section on anticoagulation
effective, and generally safe, especially when carried out
electively. Emergent cardioversion is an uncommon event,
Chronic maintenance of SR remains the major challenge
because most patients can be rendered stable with acute rate
in this realm. To date, we have not seen the development of
control and measures to treat an underlying disease process.
any antiarrhythmic drug with sufficient efficacy and safety
This is fortunate, because patients frequently are not pre-
to allow us to administer it with confidence to a broad sam-
pared properly for cardioversion, having recently eaten and
ple of patients. It is important to remember that even with
not being properly anticoagulated. In addition, emergent car-
optimal therapy, drug treatment is rarely “curative.” In most
dioversion is plagued with a very high relapse rate because
cases, the most we should expect is a reduction in the fre-
the conditions that led to the arrhythmia still are present.11,12
quency, duration, and severity of the events, which may be
For elective cardioversion, with good technique including the
adequate in some patients to improve their quality of life
use of biphasic waveform devices and adequate anesthesia,
and to allow them to pursue their usual activities.32 In addi-
>95% of patients can be shocked into SR.13-15 Unfortunately,
tion, antiarrhythmic drugs have the potential for toxicity. The
early recurrence of AF and late relapses are not uncommon
best we have been able to do is to describe safety and effi-
and occur as a consequence of concomitant cardiac or elec-
cacy in carefully defined patient populations to allow physi-
trical disease and other factors, the most important of which
cians to prescribe one or another agent depending on the
may be the duration of the antecedent arrhythmia.16,17 Pre-
individual patient profile. For example, it is important to dis-
vention of early or late relapses usually requires predosing
tinguish between paroxysmal and persistent AF, because the
with antiarrhythmic drugs or beta-blockers.5,6,11,12,18,19
former frequently causes severe symptoms in young active
Management of Atrial Fibrillation
disease in order to be able to provide physicians with the bestprescribing information.
Finally, it is important to note that nonantiarrhythmic
drugs may play an important role in rhythm control. For manyof these agents, the magnitude of the treatment effect may bemodest, but if applied to a very large at-risk population, thedividends could be significant. For example, emerging datasuggest that drugs that interfere with the renin-angiotensinsystem may limit atrial fibrosis and at the same time reducethe frequency of AF when used in patients after myocardialinfarction. Widespread use of these agents, which also con-trol hypertension, the most common cause of AF, would beexpected to reduce the disease burden.36 Studies to confirmthis benefit are in progress. Figure 2. A pharmacologic approach to maintenance of sinus rhythm, as Rate Versus Rhythm Control previously published in the ACC/AHA/ESC guidelines.10 (Reproduced withpermission from Fuster V, Ryden LE, Asinger RW, et al.; American College
The lack of highly effective and safe antiarrhythmic drugs
of Cardiology/American Heart Association Task Force on Practice Guide-
prompted several investigators to ask the question whether
lines; European Society of Cardiology Committee for Practice Guidelines
maintenance of SR is actually preferable to allowing AF
and Policy Conferences (Committee to Develop Guidelines for the Manage-
to persist. Obviously, the question is valid only for patients
ment of Patients with Atrial Fibrillation); North American Society of Pac-
who have minimal or no symptoms while in rate-controlled
ing and Electrophysiology: ACC/AHA/ESC guidelines for the management
AF, because severe symptoms would prompt the physician
of patients with atrial fibrillation: Executive summary. Circulation 2001;
to recommend rhythm reversion. It should be clear that this
is not a new idea. For decades, experienced clinicians al-lowed AF to persist, based on the premise that antiarrhythmicdrugs are not safe, particularly in the elderly, and could placethe patient in more danger than the arrhythmia itself.37,38
individuals whereas the latter may become less noticed and
For example, all antiarrhythmic drugs depress the conduc-
more amenable to a conservative strategy of rate control only.
tion system, including the sinoatrial node, and many patients
The latest guidelines issued by our professional organizations
with AF have concomitant conduction disease. Thus, insis-
have grouped patients by type of heart disease and presented
tence on maintenance of SR could mandate a pacemaker
what might be considered first-line and alternative drug ther-
implantation, which would be avoided if AF is allowed to
apy based on that classification (Fig. 2).10 For example, in
the realm of congestive heart failure, the drugs best studied
Four randomized studies that have been completed and re-
for efficacy and safety are clearly dofetilide and amiodarone,
ported have examined this question.39-41 Although the studies
which makes those two agents the preferred therapy for pa-
are of varying size and used different methods and endpoints,
tients with severe left ventricular dysfunction. It appears from
the overwhelming message from all of them is that, aside from
good trial data that neither drug is associated with deterio-
symptom control, there does not appear to be an advantage
ration of left ventricular function in these patients, nor does
for rhythm control in terms of quality of life, mortality, hos-
either agent predispose patients to lethal proarrhythmia once
pitalization rates, or any other endpoint examined.41 In fact,
they have been started carefully and as long as rigid dosing
in many of the analyses, the advantage went to the more sim-
guidelines are adhered to. Similarly, sotalol, dofetilide, and
ple strategy of rate control. Although there are a number of
amiodarone are featured for patients with ischemic heart dis-
caveats in the interpretation of these data (including patient
ease based on good data from randomized clinical trials that
selection bias, inefficiencies in SR retention, and relatively
the drugs were safe in such patients, and with effectiveness
short follow-up periods), it is now axiomatic that letting el-
not diminished in comparison to patients without coronary
derly patients remain in SR for a few years is not inimical
artery disease.33-35 Many more agents have been examined
to their outcome and may be preferred to exposing those in-
in patients with normal hearts, multiplying the therapeutic
dividuals to the hazards of antiarrhythmic drug therapy and
alternatives for those patients. Although highly useful for
repeated cardioversions. Although some of these randomized
clinical purposes, schema such as these point out the limi-
trials permitted nonpharmacologic therapy for SR mainte-
tations of the chemical agents currently on the market and
nance, too few of those patients were so treated to allow any
the need for better comparative information. It also is clear
conclusions as to whether a nondrug approach would alter
that we need better antiarrhythmic drugs with less attendant
cardiac and organ toxicity. In fact, several new agents are un-der active investigation that have greater specificity for atrialelectrophysiology or have novel mechanisms of action to cir-
Anticoagulation
cumvent the problems engendered by blocking standard ioncurrents. Whether these agents will make it to market and
By far, the most important issue in AF management is an-
what impact they will have on AF management remain to
ticoagulation.10,42 It now is clear that avoidance of stroke ren-
be seen.6 It is clear that new antiarrhythmic drugs will be
ders AF treatment an exercise in symptom reduction rather
held to a high standard of safety and will need to be studied
than an attempt to preserve life and prevent major disabil-
comprehensively in patients with a broad spectrum of cardiac
ity. Fortunately, a number of large, well-done clinical trials
Journal of Cardiovascular Electrophysiology Vol. 14, No. 12, Supplement, December 2003
Anticoagulation Trials in Atrial Fibrillation
Reference Year Published No. of Patients Interventions
Copenhagen Atrial Fibrillation, Aspirin, Anticoagulation I (AFASAK I)
Copenhagen Atrial Fibrillation, Aspirin, Anticoagulation II (AFASAK II)
Stroke Prevention in Atrial Fibrillation I (SPAF I)
Stroke Prevention in Atrial Fibrillation II (SPAF II)
Stroke Prevention in Atrial Fibrillation Ill (SPAF Ill)
Boston Area Anticoagulation Trial for Atrial Fibrillation (BAATAF)
Canadian Atrial Fibrillation Anticoagulation (CAFA)
Stroke Prevention in Nonrheumatic Atrial Fibrillation (SPINAF)
European Atrial Fibrillation Trial (EAFT)
Studio ltaliano Fibrillazione Atriale (SIFA)
Minidose Warfarin in Nonrheumatic Atrial Fibrillation
Prevention of Arterial Thromboembolism in Atrial Fibrillation (PATAF)
Low-dose Aspirin, Stroke, Atrial Fibrillation (LASAF)
European Stroke Prevention Study II (ESPS II)
French Aspirin Coumarin Collaborative Study
Stroke Prevention using an Oral Thrombin Inhibitor in
AF = atrial fibrillation; ASA = aspirin; LMW = low molecular weight; OA = oral anticoagulation; OA∗ = low-dose oral anticoagulation. Adapted and reproduced with permission from Hart RG, Benavente O, McBride R, Pearce LA: Antithrombotic therapy to prevent stroke in patients withatrial fibrillation: A meta-analysis. Ann Intern Med 1999;131:492-501.
have proven that warfarin is effective in dramatically reduc-
It is very clear that risk for stroke in AF can be quanti-
ing the incidence of thromboembolic events in patients with
fied based on a number of clinical characteristics, including
valvular and nonvalvular AF (Table 1).10,42 Warfarin, how-
age, sex, cardiac function, and associated clinical conditions
ever, is a complex drug, and the incidence of major bleeding
such as diabetes and hypertension (Table 1).10,47,48 For high-
associated with its use is not inconsequential. Thus, physi-
risk individuals, we now believe that warfarin anticoagulation
cian and patient acceptance and its applicability to high-risk
should never be discontinued once initiated. This recommen-
populations have all been major issues limiting its general
dation comes from several lines of evidence. We know that
application. In addition, strict guidelines must be followed at
many patients do not know when they are having AF. Asymp-
each phase of the disease’s management in order to obtain
tomatic relapses may predispose to stroke. In fact, the first
the benefits that have been described in clinical trials. For
presenting symptom of AF is stroke in a sizable percentage
example, patients with recent-onset arrhythmia (<48 hours)
of elderly patients.49 Recently, the randomized studies of rate
must have a continuously therapeutic level of anticoagula-
versus rhythm control reported a disturbingly high incidence
tion (international normalized ratio [INR] >2.0) for 3 to 4
of strokes in patients in the rhythm control arm of the trials
weeks prior to an elective drug or electrical conversion.10,43
whose anticoagulation either was stopped or was at an inad-
Alternatively, such patients may undergo a transesophageal
equate level.40 The reason for this is not clear but could have
echocardiogram and simultaneous anticoagulation with hep-
been due to AF recurrences during which symptoms were
arin followed by warfarin and cardioversion if the study indi-
masked by drugs that slow the ventricular response to AF
cates the absence of left atrial clot.44,45 Although the studies
if they do not suppress it, rendering stroke more likely. In
supporting these recommendations were not necessarily well
any case, guidelines that in the past advocated cessation of
controlled or randomized, their results are well accepted and
anticoagulation in patients maintaining SR for several weeks
after conversion may have to be restricted to patients who
Chronic anticoagulation is a more complex issue. First, it
have AF without stroke risk factors.
is clear that aspirin, although effective, is grossly inferior to
What also is clear is that warfarin alternatives are desper-
warfarin for this indication and should be used only in patients
ately needed. To date, evidence supporting the efficacy of
who cannot take warfarin.10 Although routinely used in “low-
alternative therapy has been lacking. Heparins, including re-
risk” patients, the rationale for this practice is nil. Patients
cently some low-molecular-weight heparins, have been found
with atrial flutter require warfarin anticoagulation, as do AF
useful in association with the transesophageal cardioversion
patients based on their relative risks of atrial clot formation
strategy discussed earlier, but they have not been well studied
and stroke in large series.46 Although we try to differentiate
otherwise.50,51 The need for parenteral administration greatly
risk based on AF burden, there are no data concluding that
diminishes their clinical applicability in any case. Recently,
patients with paroxysmal AF are at less risk for stroke than
we have seen encouraging results from trials in which di-
patients with persistent AF. Whether relative frequency of
rect thrombin inhibitors have been compared with warfarin
AF within the paroxysmal category is a risk stratifier has not
in patients with nonvalvular AF.52 These drugs have the po-
tential advantage of a shorter half-life, permitting faster onset
Management of Atrial Fibrillation
and offset, fewer drug interactions, and empiric dosing with-
11. Villani GQ, Piepoli MF, Terracciano C, Capucci A: Effects of dilti-
out the need for monitoring coagulation status. Given the
azem pretreatment on direct-current cardioversion in patients with per-
dire nature of the clinical outcomes in these trials, placebo
sistent atrial fibrillation: A single-blind, randomized, controlled study. Am Heart J 2000;140:437-443.
controls are not possible. Positive controlled studies versus
12. Marcus GM, Sung RJ: Antiarrhythmic agents in facilitating electrical
warfarin, even those with a noninferiority endpoint, mandate
cardioversion of atrial fibrillation and promoting maintenance of sinus
the inclusion of a very large number of at-risk patients, with
double dummy and phantom INR-based dose adjustments
13. Page RL, Kerber RE, Russell JK, Trouton T, Waktare J, Gallik D,
Olgin JE, Ricard P, Dalzell GW, Reddy R, Lazzara R, Lee K, Carl-
and scrupulous safety monitoring. The ability to use sim-
son M, Halperin B, Bardy GH; BiCard Investigators: Biphasic versus
pler drugs for this indication would have far-reaching con-
monophasic shock waveform for conversion of atrial fibrillation: The
sequences and could revolutionize our approach to patients
results of an international randomized, double-blind multicenter trial. J
with low-to-intermediate risk of stroke, including those with
compliance issues. The preliminary results have been very
14. Havranek E: Biphasic waveform shocks were effective and efficient for
cardioversion of atrial fibrillation. ACP J Club 2003;138:8.
encouraging, and we anticipate that anticoagulation of pa-
15. Ermis C, Zhu AX, Sinha S, Iskos D, Sakaguchi S, Lurie KG, Benditt
tients with AF soon will be simplified.
DG: Efficacy of biphasic waveform cardioversion for atrial fibrillationand atrial flutter compared with conventional monophasic waveforms. Conclusion
16. Alt E, Ammer R, Lehmann G, Putter K, Ayers GM, Pasquantonio
Management of AF is a highly complex task that requires a
J, Schomig A: Patient characteristics and underlying heart disease
thorough knowledge of several therapeutic alternatives, care-
as predictors of recurrent atrial fibrillation after internal and exter-
ful individualization of therapy, and patience on the part of the
nal cardioversion in patients treated with oral sotalol. Am Heart J1997;134:419-425.
physician and patient. The search for better treatment alter-
17. Ortiz De Murua JA, del Carmen Avila M, Ochoa C, de La Fuente L,
natives continues because of the burden of this arrhythmia in
Morena De Vega JC, del Campo F, Villafranca JL: Independent predic-
our population and the limitations of what is currently avail-
tive factors of acute and first year success after electrical cardioversion
able. Although many of these new treatments will come to
in patients with chronic atrial fibrillation. Rev Esp Cardiol 2001;54:958-964.
fruition, AF will remain a challenge for clinicians for years to
18. Miller MR, McNamara RL, Segal JB, Kim N, Robinson KA, Goodman
come. It deserves the attention it has received and will receive
SN, Powe NR, Bass EB: Efficacy of agents for pharmacologic conver-
from the scientific and clinical communities.
sion of atrial fibrillation and subsequent maintenance of sinus rhythm:A meta-analysis of clinical trials. J Fam Pract 2000;49:1033-1046.
19. Dayer M, Hardman SM: Special problems with antiarrhythmic drugs
Acknowledgment: The authors thank Rose Marie Wells for her usual patient
in the elderly: Safety, tolerability, and efficacy. Am J Geriatr Cardiol
help in the preparation of the manuscript.
20. Wijffels MC, Dorland R, Allessie MA: Pharmacologic cardioversion
References
of chronic atrial fibrillation in the goat by class IA, IC, and III drugs:A comparison between hydroquinidine, cibenzoline, flecainide, and d-
1. Yadav A, Scheinman M: Atrial fibrillation in the elderly. Am J Geriatr
sotalol. J Cardiovasc Electrophysiol 1999;10:178-193.
21. Alp NJ, Bell JA, Shahi M: Randomised double blind trial of oral versus
2. Cain ME: Atrial fibrillation-rhythm or rate control. N Engl J Med
intravenous flecainide for the cardioversion of acute atrial fibrillation.
3. Crijns HJ, Van den Berg MP, Van Gelder IC, Van Veldhuisen DJ: Man-
22. Khan IA: Oral loading single dose flecainide for pharmacological car-
agement of atrial fibrillation in the setting of heart failure. Eur Heart J
dioversion of recent-onset atrial fibrillation. Int J Cardiol 2003;87:121-
4. Matalka MS, Deedwania PC: Atrial fibrillation in patients with heart
23. Foster RH, Wilde MI, Markham A: Ibutilide: A review of its pharma-
failure: Pharmacologic options. Congest Heart Fail 2001;7:22-29.
cological properties and clinical potential in the acute management of
5. Reiffel JA: Drug choices in the treatment of atrial fibrillation. Am J
atrial flutter and fibrillation. Drugs 1997;54:312-330.
24. Eversole A, Hancock W, Johns T, Lopez LM, Conti CR: Ibutilide: Ef-
6. Nattel S, Khairy P, Roy D, Thibaut B, Guerra P, Talajic M, Dubuc M:
ficacy and safety in atrial fibrillation and atrial flutter in a general car-
New approaches to atrial fibrillation management: A critical review of
diology practice. Clin Cardiol 2001;24:521-525.
a rapidly evolving field. Drugs 2002;62:2377-2397.
25. Kowey PR, VanderLugt JT, Luderer JR: Safety and risk/benefit analysis
7. Lamaison D, Laureille B: Antiarrhythmic treatments of permanent atrial
of ibutilide for acute conversion of atrial fibrillation/flutter. Am J Cardiol
fibrillation. Rev Prat 1993;43:1523-1531.
8. Tepper D: Frontiers in congestive heart failure: Tachycardia-related car-
26. Howard PA: Ibutilide: An antiarrhythmic agent for the treatment of atrial
diomyopathy: A common cause of ventricular dysfunction in patients
fibrillation or flutter. Ann Pharmacother 1999;33:38-47.
with atrial fibrillation referred for atrioventricular ablation. Congest
27. Gowda RM, Punukollu G, Khan IA, Patlola RR, Tejani FJ, Cosme-
Thormann BF, Vasavada BC, Sacchi TJ: Ibutilide-induced long QT
9. Aslam MS, Brookfield L: Difficult cases in heart failure: Reversible car-
syndrome and torsade de pointes. Am J Ther 2002;9:527-529.
diomyopathy due to atrial fibrillation in a 46-year-old patient. Congest
28. Singh S, Zoble RG, Yellen L, Brodsky MA, Feld GK, Berk M, Billing
CB Jr: Efficacy and safety of oral dofetilide in converting to and main-
10. Fuster V, Ryden LE, Asinger RW, Cannom DS, Crijns HJ, Frye RL,
taining sinus rhythm in patients with chronic atrial fibrillation or atrial
Halperin JL, Kay GN, Klein WW, Levy S, McNamara RL, Prystowsky
flutter: The Symptomatic Atrial Fibrillation Investigative Research on
EN, Wann LS, Wyse DG, Gibbons RJ, Antman EM, Alpert JS, Faxon
Dofetilide (SAFIRE-D) study. Circulation 2000;102:2385-2390.
DP, Fuster V, Gregoratos G, Hiratzka LF, Jacobs AK, Russell RO,
29. Al-Dashti R, Sami M: Dofetilide: A new class III antiarrhythmic agent.
Smith SC Jr, Klein WW, Alonso-Garcia A, Blomstrom-Lundqvist C,
de Backer G, Flather M, Hradec J, Oto A, Parkhomenko A, Silber S,
30. Kowey PR, Marinchak RA, Rials SJ, Filart RA: Acute treatment of atrial
Torbicki A; American College of Cardiology/American Heart Associa-
fibrillation. Am J Cardiol 1998;81:16C-22C.
tion Task Force on Practice Guidelines; European Society of Cardiology
31. Cybulski J, Danielewicz H, Kulakowski P, Budaj A, Maciejewicz J,
Committee for Practice Guidelines and Policy Conferences (Commit-
Kawka-Urbanek T, Ceremuzynski L: Intravenous amiodarone in con-
tee to Develop Guidelines for the Management of Patients with Atrial
version of new-onset atrial fibrillation. (Abstract) J Am Coll Cardiol
Fibrillation); North American Society of Pacing and Electrophysiol-
ogy: ACC/AHA/ESC Guidelines for the Management of Patients with
32. Dorian P, Paquette M, Newman D, Green M, Connolly SJ, Talajic M,
Atrial Fibrillation: Executive Summary. Circulation 2001;104:2118-
Roy D: Quality of life improves with treatment in the Canadian Trial of
Atrial Fibrillation. Am Heart J 2002;143:984-990. Journal of Cardiovascular Electrophysiology Vol. 14, No. 12, Supplement, December 2003
33. Wong CK, White HD, Wilcox RG, Criger DA, Califf RM, Topol EJ,
for stroke in type 2 diabetes mellitus: United Kingdom Prospective
Ohman EM, GUSTO-III Investigators: Management and outcome of
Diabetes Study (UKPDS) 29. Arch Intern Med 1999;159:1097-1103.
patients with atrial fibrillation during acute myocardial infarction: The
49. Wolf PA, Abbott RD, Kannel WB: Atrial fibrillation: A major contrib-
GUSTO-III experience. Global Use of Strategies To Open Occluded
utor to stroke in the elderly. The Framingham Study. Arch Intern Med
Coronary Arteries. Heart 2002;88:357-362.
34. Dofetilide in patients with left ventricular dysfunction and either heart
50. Murray RD, Deitcher SR, Klein AL: Use of low-molecular-weight hep-
failure or acute myocardial infarction: Rationale, design, and patient
arin as bridge anticoagulation therapy in patients with atrial fibrillation
characteristics of the DIAMOND studies. Danish Investigations of Ar-
undergoing transoesophageal echocardiography guided cardioversion.
rhythmia and Mortality ON Dofetilide. Clin Cardiol 1997;20:704-710.
35. Pedersen OD, Bagger H, Keller N, Marchant B, Kober L, Torp-Pedersen
51. Wodlinger AM, Pieper JA: Low-molecular-weight heparin in trans-
C: Efficacy of dofetilide in the treatment of atrial fibrillation-flutter in
esophageal echocardiography-guided cardioversion of atrial fibrillation.
patients with reduced left ventricular function: A Danish Investigation
of Arrhythmia and Mortality on Dofetilide (DIAMOND) substudy. Cir-
52. SPORTIF III Investigators: Stroke prevention using the oral direct
thrombin inhibitor ximelagatran in patients with nonvalvular atrial fib-
36. Goette A, Arndt M, Rocken C, Spiess A, Staack T, Geller JC, Huth
rillation. Late breaking clinical trial session, American College of Car-
C, Ansorge S, Klein HU, Lendeckel U: Regulation of angiotensin
diology Meeting, Chicago, Illinois, April 2003.
II receptor subtypes during atrial fibrillation in humans. Circulation2000;101:2678-2681. Discussion
37. Waldo AL: Long-term pharmacologic management of atrial fibrillation
in the elderly. Am J Geriatr Cardiol 2002;11:233-244. Dr. Prystowsky: What percent of people were not enrolled
38. Essebag V, Hadjis T, Platt RW, Pilote L: Amiodarone and the risk
of bradyarrhythmia requiring permanent pacemaker in elderly patients
in AFFIRM because the clinician felt they specifically needed
with atrial fibrillation and prior myocardial infarction. J Am Coll Cardiol
Dr. Waldo: We don’t know. There were about 3,300 pa-
39. Hohnloser SH, Kuck KH: Randomized trial of rhythm or rate control
tients followed who opted not to be in AFFIRM, and two
in atrial fibrillation: The Pharmacological Intervention in Atrial Fibril-
thirds of those who opted not to participate made the deci-
lation Trial (PIAF). Eur Heart J 2001;22:801-802.
40. Wyse DG, Waldo AL, DiMarco JP, Domanski MJ, Rosenberg Y,
sion on their own. The other third did not participate because
Schron EB, Kellen JC, Green HL, Mickel MC, Dalquist JE, Corley
SD, Atrial Fibrillation Follow-up Investigation of Rhythm Management
Dr. Packer: There is a bit of a problem on the whole abla-
(AFFIRM) Investigators: A comparison of rate control and rhythm con-
tion scene because people keep coming in and thinking that
trol in patients with atrial fibrillation. N Engl J Med 2002;347:1825-1833.
after AFFIRM and RACE we shouldn’t be ablating anybody
41. Nattel S: Rhythm versus rate control for atrial fibrillation manage-
because it doesn’t matter. These are totally different patients.
ment: What recent randomized clinical trials allow us to affirm. CMAJ
Dr. Naccarelli: As an AFFIRM investigator, there may
have been some bias against randomizing the most symp-
42. Hart RG, Palacio S, Pearce LA: Atrial fibrillation, stroke, and acute
tomatic patients. However, a number of the patients random-
antithrombotic therapy: Analysis of randomized clinical trials. Stroke2002;33:2722-2727.
ized in our center were very symptomatic. Some of these
43. Gallagher MM, Hennessy BJ, Edvardsson N, Hart CM, Shannon MS,
very symptomatic patients were randomized to rate control
Obel OA, Al-Saady NM, Camm AJ: Embolic complications of direct
and subjectively did well with complete abolition of their
current cardioversion of atrial arrhythmias: Association with low inten-
symptoms. However, rate control is probably not for every-
sity of anticoagulation at the time of cardioversion. J Am Coll Cardiol2002;40:926-933.
body, and there is a large group of patients who probably
44. Klein AL, Grimm RA, Murray RD, Apperson-Hansen C, Asinger RW,
are not candidates for rate control and may be for pharma-
Black IW, Davidoff R, Erbel R, Halperin JL, Orsinelli DA, Porter TR,
cologic suppression or even nonpharmacologic abolition of
Stoddard MF, Assessment of Cardioversion Using Transesophageal
Echocardiography Investigators: Use of transesophageal echocardio-
Dr. Packer: I’m not even going as far as saying that they’re
graphy to guide cardioversion in patients with atrial fibrillation. N EnglJ Med 2001;344:1411-1420.
not a candidate for rate control. We don’t know about those
45. Manning WJ, Silverman DI, Seto TB, Weigner MJ: Value of precar-
dioversion transesophageal echocardiography in managing cardiover-
Dr. Prystowsky: My own approach is to control the heart
sion in atrial fibrillation. J Am Coll Cardiol 2002;40:1889-1890.
rate before making a decision on symptoms. But often pa-
46. Schmidt H, von der Recke G, Illien S, Lewalter T, Schimpf R, Wolpert
Becher H, Luderitz B, Omran H: Prevalence of left atrial chamber and
tients have their rate well controlled by the time they are
appendage thrombi in patients with atrial flutter and its clinical signifi-
referred to me, and they are still quite symptomatic and want
cance. J Am Coll Cardiol 2001;38:778-784.
to be in sinus rhythm. The message of AFFIRM for me is if
47. Wehinger C, Stollberger C, Langer T, Schneider B, Finsterer J: Eval-
a person is in an older age group, they can have an option
uation of risk factors for stroke/embolism and of complications due
of rate control. We shouldn’t forget that we have minimal
to anticoagulant therapy in atrial fibrillation. Stroke 2001;32:2246-2252.
data on younger patients without a high stroke risk regarding
48. Davis TM, Millns H, Stratton IM, Holman RR, Turner RC: Risk factors
GENERAL OVERVIEW OF THE GROUP HISTORY AND DEVELOPMENT Mr. Lok, the founder of the Group, commenced his career in the development of system softwarein the 1980s and was subsequently engaged in the development and sale of customized systemsoftware in Hong Kong. In 1986, recognising the huge market potential for enterprise applicationsoftware, he started to concentrate his efforts on the deve
J. Tirapu-Ustárroz a, G. Pérez-Sayes a, M. Erekatxo-Bilbao a, C. Pelegrín-Valero b Resumen. Introducción. El cerebro es, básicamente, una máquina predictiva encaminada a reducir la incertidumbre del en- torno. El origen del concepto de ‘teoría de la mente’ se encuentra en los trabajos pioneros de Premack y Woodruf y se refiere a la habilidad para comprender y predecir la conduct
 Journal of Cardiovascular Electrophysiology
Journal of Cardiovascular Electrophysiology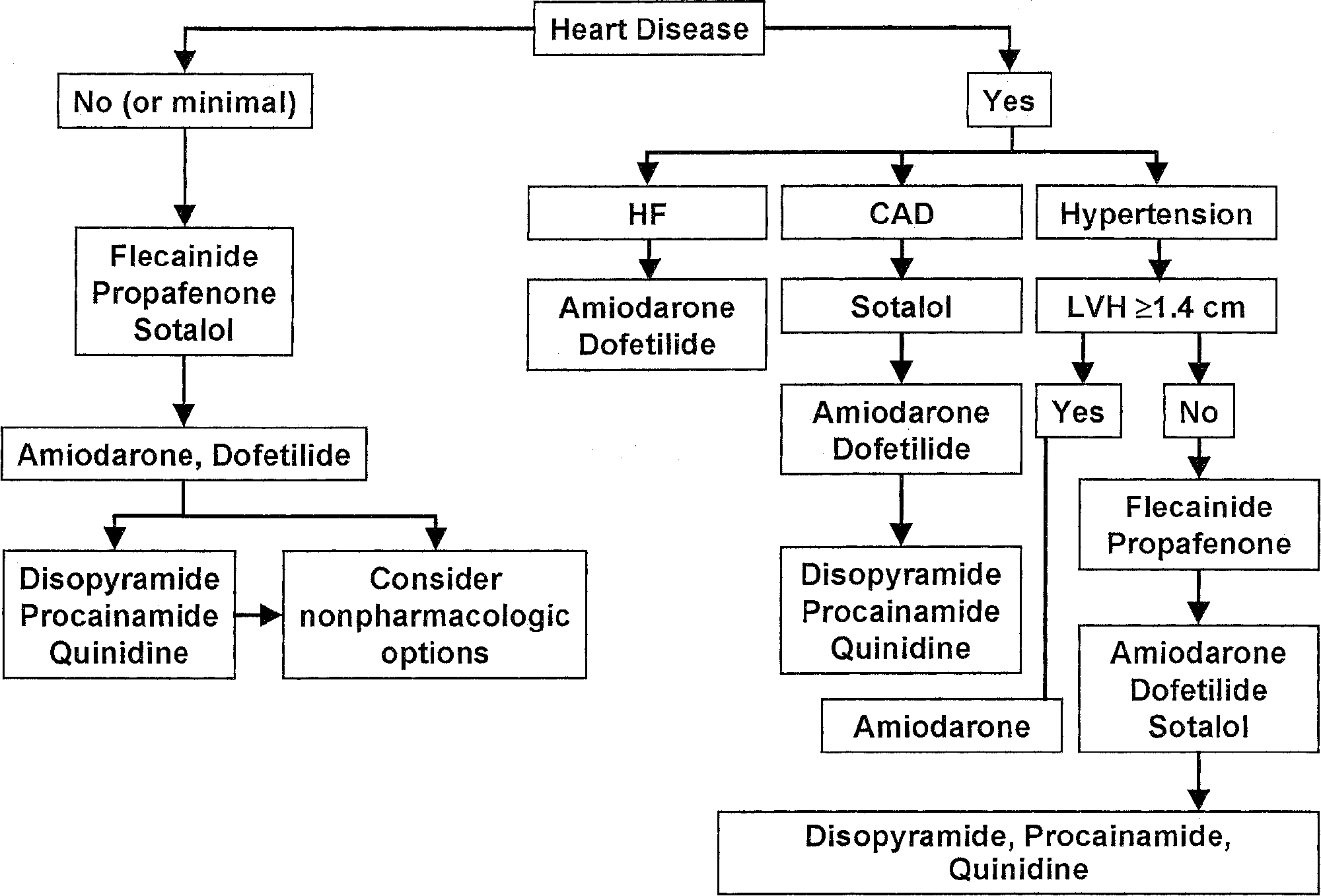 Management of Atrial Fibrillation
Management of Atrial Fibrillation